Ashley Ann Dilip1, Aswathi Anil1, Athira Antony1, Reshmi Rajan1, Soumya Mary Alex1*, Binu Upendran2
1Department of Pharmacy Practice, St.Joseph’s College of Pharmacy, Cherthala – 688524, Alappuzha, India
2Department of Nephrology, Lourdes Hospital, Kochi – 682012, India
*Address for Correspondence to Author:
Soumya Mary Alex
Assistant Professor
Dept. of Pharmacy Practice
St. Joseph’s College of Pharmacy, Cherthala – 688524, Alappuzha, India
Abstract
Sepsis can be a life-threatening organ dysfunction caused by a dysregulated host response to infection. Majority of the Indian sepsis study is done in the pediatric age groups, only limited studies on adult population. The study aimed to evaluate the management of sepsis and its adherence to the Surviving Sepsis Campaign (SSC) International Guidelines 2016. This cross-sectional study (Ambispective, single-center) is being done by taking details of patients from the medical records and the Mediware system available in a tertiary care hospital, Ernakulam. A total of 320 patients, among which 117 were analysed prospectively and 203, retrospectively. The management of sepsis is done thoroughly with timely fluid therapy, antimicrobial therapy, blood component and vasopressor therapy. Adherence to SSC Guidelines-2016 (both 3-Hour and 6-Hour bundles) was found to be 57.5%. While categorizing the “Stages of Sepsis" the incidence of “sepsis” was found to be higher. Urinary Tract Infection-141 (44.06%) was the most predominent focus of infection in which E.COLI-71 (22.18%) was the frequently isolated pathogen. When correlating the CCI (Charlson Comorbidity Index) Score status (comorbidities) and outcome (alive or dead) significant association was observed. Then comparing the Quick Sequential Organ Failure Assessment (qSOFA) risk status (mortality) and outcome among the total patients it was found to be statistically significant. Drug interactions and untreated indications were the mostly occurred Drug Related Problems (DRPs) in prospective and retrospective analysis respectively.
Keywords: Sepsis, surviving sepsis campaign international guidelines, Charlson Comorbidity Index, quick sequential organ failure assessment, drug related problems
Introduction
Sepsis is a medical condition which describes the body’s systemic immunological response to an infection that may cause end-stage organ dysfunction and even death. Septicaemia is the acute invasion of the systemic circulation by pathogenic organism accompanied by sepsis or septic shock with possible microbial localisation in various body system (Gyawali et al., 2019). In the United States sepsis is the second most leading cause of death in non-coronary intensive care unit (ICU) patients. Sepsis is common and more dangerous in elderly, immunocompromised and critically ill patients. It occurs in 1-2% of all hospitalised patients and accounts for as many as 25% of ICU bed utilization.
Infections that cause sepsis most commonly start in the lungs, urinary tract, skin, or gastrointestinal tract. Any infection can lead to sepsis, but the infections that may have increased chance of causing sepsis are Respiratory tract infections (40%), Urinary tract infections (18%), Gastrointestinal infections (14%), kidney infections and blood poisoning (O’Connell and Vandergriendt, 2021; CDC 2022). The most common organ dysfunctions were acute respiratory distress syndrome (57 %) and acute kidney injury (46 %) (Rhodes et al., 2015).
There are three stages of sepsis: sepsis, severe sepsis and septic shock. Sepsis is two or more systemic inflammatory response criteria plus a known or suspected infection. Severe sepsis is sepsis with acute organ dysfunction. Acute organ dysfunction can manifest in any organ, and frequently manifests clinically as shock, respiratory failure, acute kidney injury, hematologic or metabolic disturbances or neurologic decline. Septic shock is a form of severe sepsis where the organ dysfunction involves the cardiovascular system. This may lead to many serious complications which including organ dysfunction, respiratory or heart failure, stroke, possible death (O’Connell and Vandergriendt, 2021).
The most common etiologic pathogens are : Gram positive bacteria (Staphylococcus aureus; Streptococcus pneumoniae, Coagulase-negative staphylococci, and enterococci ; Streptococcus pyogenes and viridans), Gram negative bacteria (E. Coli; Klebsiella spp; Serratia spp; Enterobacter spp; and Proteus spp; Pseudomonas aeruginosa), Fungi (Candida albicans; Candida tropicalis; Aspergillus ), Viruses (Adenovirus; Rhinovirus; Influenza A& B). A large proportion of patients with gram-negative bacteraemia develop clinical sepsis. Gram negative bacteria were more likely to produce septic shock in comparison with gram-positive organisms (50% Vs 25%). Gram-negative sepsis results in a higher mortality rate compared with sepsis from any other groups of organisms (Ryding and Lois Zoppi, 2018).
The European Society of Intensive Care Medicine (ESICM) apace with the Society of Critical Care Medicine (SCCM) launched the Surviving Sepsis Campaign (SSC) in 2002 with various aims comprising the development of guidelines for diagnosis, treatment, and post-ICU care of sepsis and scaling down of mortality from sepsis (Surviving Sepsis Guidelines). Without appropriate timely treatment, sepsis can rapidly lead to tissue damage, organ failure, and eventually death. Early diagnosis , timely and appropriate clinical management of sepsis, such as optimal antimicrobial use, fluid resuscitation, etc are crucial to increase the likelihood of survival. Even though the onset of sepsis can be acute and posses a short-term mortality burden, it can also be the cause of significant long-term morbidity requiring treatment and support. Thus, sepsis requires a multidisciplinary approach (CDC 2022).
Delay in antibiotic treatment could potentially have a negative effect on patient outcome, thus suggesting a need of systematic improvement in the initial management of patient with sepsis in the emergency department (Husabø et al., 2020). Pneumonia was the most common source of sepsis (32.6%), and patients with pneumonia had the highest mortality of all other subsets receiving bundle non-adherent care. Although overall mortality was lower among those who received bundle-adherent care compared to those who did not (Milano et al., 2018). There was a lower adherence to resuscitation guidelines in the group of patients over 65 with severe sepsis and septic shock when compared with the group of patients less than 65 years (Negret-Delgado et al., 2016).
Adherence to the SSC Guidelines can improve the quality of management of sepsis and decrease the mortality rate. Identifying the Drug Related Problems (DRPs) and initiating appropriate interventions can improve the quality of life. Optimization of therapy can be achieved by identifying the causative organism and categorising sepsis . Therefore, this study aimed to evaluate the management of sepsis and its adherence to the Surviving Sepsis Campaign (SSC) International Guidelines 2016.
Objectives
Materials and methods
Design of Study: A cross-sectional study (Ambispective, single-center)
Protocol: The study was approved by Institutional Ethics Committee (Reg no: ECR/482/Inst/KL/2013/RR-19 Dated 07/10/2021)
Duration of Study: 6 months (December 2021 to May 2022). The study is being done by taking details of patients from the medical records and the Mediware system available in the Lourdes Hospital, Ernakulam for a period of 6 months (1-12-2021 to 30-5-2022) prospectively and five years (01-05-2016 to 30-4-2021) retrospectively.
Study Settings: Lourde’s Hospital, Post Graduate Institute of Medical Science and Research, Ernakulam , Kochi - 682 012, Kerala , India ,which is a multi-speciality tertiary care hospital.
Sample Size: All patients who met the inclusion & exclusion criteria was selected. A total of 320 patients who satisfied the diagnostic criteria of sepsis were included in the study (Minimum sample size required was found to be 312).
Inclusion Criteria
1. Patients of both gender above 18 years satisfying at least 6 diagnostic criteria of SSC guidelines.
Exclusion Criteria
1. Patients who discharged against the medical advice.
2. Patients who expired within 72 hours of admission.
Data Collection Tool
1. Lourde’s mediware system
2. Medical records of the patients
3. Specially designed data collection form
4. PCNE DRP Classification tool V9.1
5. Naranjo ADR Probability Scale
Data Collection
The Retrospective patient demographic details, pertinent laboratory as well as treatment details were extracted from medical records and Lourde’s mediware system. Prospective data obtained from the patient files in emergency department.
Methodology
Randomly collected the patient data of both gender above 18 years satisfying at least 6 diagnostic criteria of SSC guidelines for a period of 6 months (1-10-2021 to 30-4-2022) prospectively from the emergency department and various ICU’s and five years (01-05-2016 to 30-4-2021) data retrospectively from the medical records as well as the mediware system available in the Lourdes Hospital, Kochi. The various parameters that are included in the study are Patient demographic details, Vitals, Culture and Sensitivity reports, Various Lab Investigations and the management measures taken within the initial hours of hospitalization and the Drug therapy given. Study on the effect of co morbidities, prediction of outcome using various scores [Sequential Organ Failure Assessment Score(SOFA) and Charlson Comorbidity Index Score(CCI)]) and drug related problems during the management of sepsis were also be evaluated.
Statistical Analysis
The collected data were analysed and interpreted using microsoft excel and SPSS. Frequency of various variables were found out using SPSS and excel software and were presented as graphs, tables and pie diagrams. Adherence to the SSC Guideline 2016,association between co morbidities and outcome as well as mortality and outcome were assesed using Pearson Chi-Square.
Results
Three twenty cases of sepsis cases managed in a tertiary care hospital during a period of 6 months (1-10-2021 to 30-4-2022) prospectively and five years (01-05-2016 to 30-4-2021) retrospectively were randomly studied and evaluated for management, adherence to the guideline. Categorization of sepsis and causative organisms, effect of comorbidities and prediction of outcome using various scores and drug related problems was done.
Demographics of the study population
In our study, the incidence of sepsis cases were age adjusted and it was found that elderly patients was more likely to have sepsis (58%) compared with middle aged (33%) and younger (9%) adults. Out of 320 patients, 185 (58%) were males & 135 (42%) were females.
Management of sepsis
The study evaluated the management of sepsis according to the SSC International Guidelines-2016. Fluid therapy, Antimicrobial therapy (Antibiotics & Antifungals), Vasopressor therapy, Blood component therapy were analyzed.
Fluid therapy
Depending on the patient’s clinical status different fluids like normal saline, dextrose, dextrose in normal saline (DNS) and ringer lactate (RL) were prescribed. Out of 320 patients 314 (98.13%) were treated with IV fluids, among this normal saline 283 (90.13%), ringer lactate 18 (5.73%), dextrose in normal saline 7 (2.23%), dextrose 6 (1.91%). In the prospective analysis out of 117 patients 112 (95.73%) were prescribed with IV fluids in which normal saline 103 (91.96%), dextrose 4 (3.57%), dextrose in normal saline 2 (1.79%), ringer lactate 3 (2.68%). Similarly in the retrospective analysis out of 203 patients 202 (99.51%) were prescribed with IV fluids; within this normal saline 180(89.11%), ringer lactate 15(7.42%), dextrose in normal saline 5(2.48%), dextrose 2 (0.99%).
Antimicrobial therapy
Based on the focus of infection and causative organism various antimicrobials (Antibiotics & Antifungals) were prescribed.
Antibiotic therapy
Among the various antibiotics prescribed the most commonly used class of antibiotics comprises of, cephalosporins in 206 patients (64.37%), carbapenems in 163 patients (50.93%), penicillins in 58 patients (18.13%).
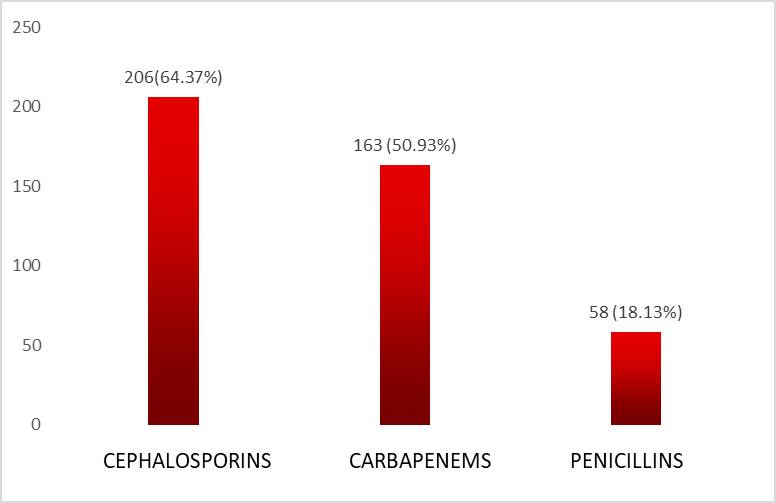
Figure 1. Cephalosporins Vs Carbapenems Vs Penicillins in study population
In the prospective and retrospective analysis, while considering the cephalosporin class of antibiotics cefoperazone-sulbactum combination therapy was the most commonly prescribed one, followed by ceftriaxone, cefixime, cefuroxime, cefotaxime, cefepime and ceftazidime.In the retrospective analysis a total of 137 (67.48%) patients were administered with cephalosporins, among cefoperazone-sulbactum (80%), cefixime (13%), ceftriaxone (12%),cefotaxime (1%) and cefepime (1%). In the prospective analysis a total of 69 (58.97%) patients were administered with cephalosporins, among which cefoperazone-sulbactum (75%), ceftriaxone (41%), cefixime (30%), cefuroxime (29%), cefotaxime (7%), cefepime (4%) and ceftazidime (1%).
The most commonly prescribed penicillin class of antibiotics was piperacillin-tazobactum and benzylpenicillin in the prospective and retrospective analysis respectively followed by amoxicillin-clavulanic acid. In the prospective analysis, out of 117 patients 17 (14.52%) patients were prescribed with penicillins and in the retrospective analysis out of 203 patients 41(20.19%) patients were prescribed with penicillins.
Carbapenems were the next commonly used class of antibiotics among which meropenm was the extensively prescribed retrospectively and prospectively followed by faropenem and imipenem. In the prospective analysis out of 117 patients 70 (59.8%) patients were prescribed with carbapenemsand in the retrospective analysis out of 203 patients, 93(45.81%) patients were prescribed with carbapenems.
While considering the overall antibiotics prescribed (a total of 605 antibiotics in 320 patients), cefoperazone-sulbactum (50.63%) was the most frequently prescribed antibiotic which belongs to the class third generation cephalosporins.
Table 1. Class wise distribution of antibiotic therapy in study population
|
Treatment |
Frequency |
Percentage |
|
CEPHALOSPORINS Cefoperazone-Sulbactum Ceftriaxone Cefixime Cefuroxime Cefotaxime Cefepime Ceftazidime |
162 45 40 34 7 4 1 |
50.63% 14.06% 12.50% 10.63% 2.19% 1.25% 0.31% |
|
PENICILLINS Benzylpenicillin Piperacillin-Tazobactum Amoxicillin-Clavulanic acid |
22 16 14 |
6.87% 5.00% 4.37% |
|
CARBAPENEMS Meropenem Faropenem Imipenem |
104 15 2 |
32.50% 4.68% 0.63% |
|
NITROIMIDAZOLE Metronidazole |
47 |
14.68% |
|
MACROLIDE Clarithromycin |
20 |
6.25% |
|
LINCOMYCIN Clindamycin |
15 |
4.68% |
|
AMINOGLYCOSIDE Amikacin Gentamycin Tobramycin |
12 3 2 |
3.75% 0.93% 0.63% |
|
GLYCOPEPTIDES Vancomycin Teicoplanin Colistin |
6 3 9 |
1.87% 0.93% 2.81% |
|
FLUOROQUINOLONES Ciprofloxacin Levofloxacin Ofloxacin |
3 3 3 |
0.93% 0.93% 0.93% |
|
TETRACYCLINES Doxycycline Minocycline |
2 1 |
0.63% 0.31% |
|
OTHERS Nitrofurantoin Linezolid Rifaximin |
2 5 3 |
0.63% 1.56% 0.93% |
Antifungal therapy
Focusing on the antifungal therapy out of 320 patients 47(14.68%) patients were prescribed -with antifungals which includes fluconazole-30 (64%), clotrimazole-6 (13%), voriconazole 5 (11%), itraconazole-5 (10%) and miconazole-1 (2%).
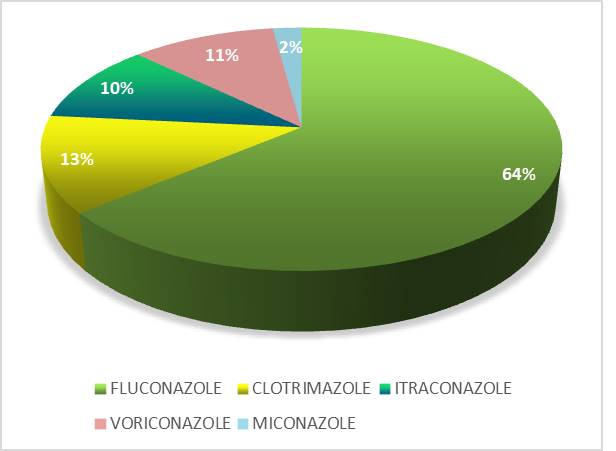
Figure 2. Overall antifungal therapy in study population
Fluconazole was the frequently used antifungal agent in both prospective and retrospective analysis. In the prospective analysis 13 patients were prescribed with antifungals, the proportion of different antifungals are fluconazole (55%), itraconazole (15%), voriconazole (15%) and clotrimazole (15%), Similarly in retrospective analysis 34 patients were given antifungals and the proportion was fluconazole (68%), clotrimazole (11%), voriconazole (9%), itraconazole (9%) and miconazole (3%).
In this study only the azole group antifungals had been prescribed.
Vasopressor therapy
Taking into consideration the vasopressor therapy, noradrenaline was predominantly prescribed then adrenaline and dopamine. Out of 320 patients 73(22.81%) were prescribed with vasopressor therapy. In the prospective analysis a total of 22 patients were administered with noradrenaline (75.86%), similarly in retrospective analysis the same was prescribed for 27 patients (61.36%).
Blood component therapy
Blood component therapy was considered if the tissue hypoperfusion has resolved and in the absence of uncontrolled situations like CAD, acute hemorrhage, lactic acidosis etc.
In our study, out of 320 patients 149 (46.56%) patients received blood component therapy which includes PRBC (84%) and FFP (16%).
During the analysis it was found that PRBC was the most broadly used blood component in both prospective and retrospective studies.
Adherence to the guideline
This study is according to the Surviving Sepsis Campaign (SSC) international guidelines 2016, which includes 2 bundles ie,3 hour and 6 hour bundles.
In the 3 hour bundle, to be completed within 3 hours include lactate level, obtaining blood cultures prior to administration of antibiotics, administering broad spectrum antibiotic, administering 30ml/kg crystalloids for hypotension or lactate ≥ 4mmol/l
In the 6 hour bundle, to be completed within 6 hours include administering vasopressors to maintain a MAP ≥65mmHg,in the event of persistent arterial hypotension despite volume resuscitation on initial lactate ≥4mmol/l:measure CVP and ScvO₂,remeasure lactate if initial lactate was elevated.
3-Hour bundle adherence
In the prospective analysis out of 117 patients, studied measurement of lactate within 3 hours was carried out in only 85 patients, obtained the blood culture prior to antibiotic administration for 114 patients, then broad spectrum antibiotics was administered for 117 and crystalloids were adminstered for 107 patients.
In the retrospective analaysis out of 203 patients, lactate measurement was done in 137 patients,blood culture prior to antibiotics administration obtained for 194 patients,broad spectrum antibiotics provided for 203 and crystalloids were administered for 191 patients.
On analysing the 3 hour complaince 64.1% and 60.6% adherence to the guideline in the prospective and retrospective analysis respectively and totally 61.9% adherence was found.
6-hour bundle adherence
While considering the 6 hour compliance in the prospective analysis 29 patients were prescribed with vasopressors, in the event of persistent arterial hypotension none of the patients were assessed for CVP and ScVO₂, and remeasurement of lactate was done in 81 patients. Similarly in retrospective analysis 44 patients were prescribed with vasopressors, none of the patients were assessed for CVP and ScVO₂, and finally remeasurement of lactate was done in 132 patients.
On evaluating the 6 hour compliance 87.2% and 84.2% adherence to the guideline was identified in the prospective and retrospective analysis respectively and as a whole, it is 85.3%.00.
Table 2. Prospective Vs Retrospective analysis of 3-HOUR compliance
|
3-Hour Compliance |
|||
|
Study Design |
Frequency |
Percent |
|
|
Prospective |
No |
42 |
35.9% |
|
Yes |
75 |
64.1% |
|
|
Total |
117 |
100.0% |
|
|
Retrospective |
No |
80 |
39.4% |
|
Yes |
123 |
60.6% |
|
|
Total |
203 |
100.0% |
|
|
Total |
No |
122 |
38.1% |
|
Yes |
198 |
61.9% |
|
|
Total |
320 |
100.0% |
|
Table 3. Prospective Vs Retrospective analysis 6-HOUR compliance
|
6-Hour Compliance |
|||
|
Study Design |
Frequency |
Percent |
|
|
Prospective |
NO |
15 |
12.8% |
|
YES |
102 |
87.2% |
|
|
Total |
117 |
100.0% |
|
|
Retrospective |
NO |
32 |
15.8% |
|
YES |
171 |
84.2% |
|
|
Total |
203 |
100.0% |
|
|
Total |
NO |
47 |
14.7% |
|
Yes |
273 |
85.3% |
|
|
Total |
320 |
100.0% |
|
Subjective to our analysis out of 320 patients 184(57.5%) were checked with both 3 hour and 6 hour compliance.
Categorization of sepsis
Out of 320 patients the incidence of sepsis-137 (43%) was greater when compared with the severe sepsis-128 (40%) and septic shock-55 (17%)
Table 4. Categorization of sepsis Prospective Vs Retrospective analysis
|
Sepsis Category |
Prospective |
Retrospective |
||
|
Frequency |
Percentage |
Frequency |
Percentage |
|
|
Sepsis Severe Sepsis Septic Shock Total |
55 |
47.0 |
82 |
40.4 |
|
44 |
37.6 |
84 |
41.4 |
|
|
18 |
15.4 |
37 |
18.2 |
|
|
117 |
100.0 |
203 |
100.0 |
|
In the prospective analysis among the three categories, sepsis had higher rate of occurence than severe sepsis and septic shock.
Causative organism
In our study bacteria was the most commonly identified causative organism.
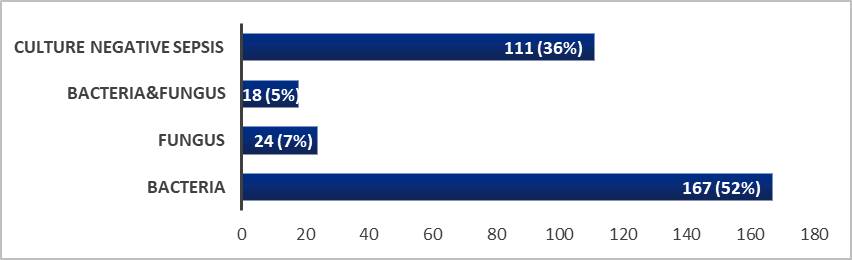
Figure 3. Different causative organisms in study population
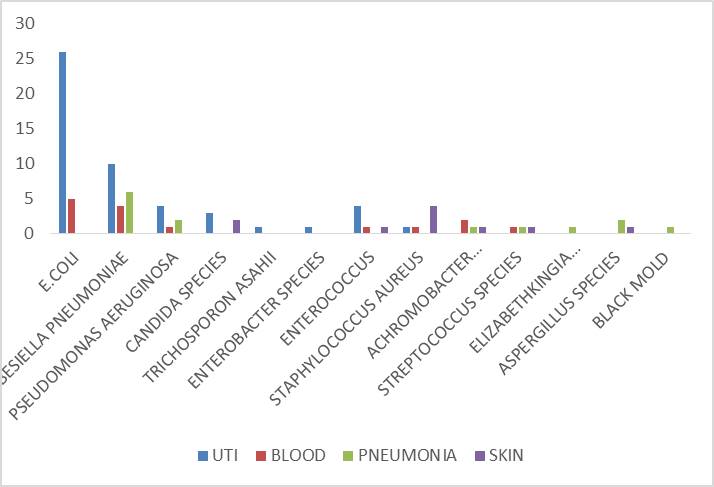
Figure 4. Prospective analysis of Organism Vs Focus of infection
While considering both prospective and retrospective analysis based on the focus of infection UTI-141(44.06%) was the most predominent one in which E.COLI-71(22.18%) was the frequently isolated pathogen.
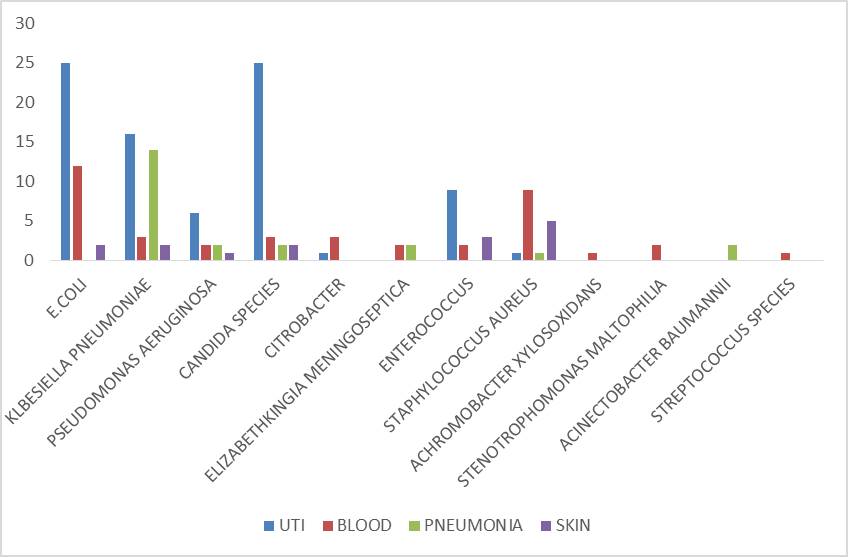
Figure 5. Retrospective analysis of Organism Vs Focus of infection
Effect of comorbidities and prediction of outcome using various scores
In our study for assessing the effect of comorbidities and mortalilty rate we used two scoring systems such as Charlson Comorbidity Index (CCI) and qSOFA.
CCI consisting of 17 items one of which is the patient age and the others are comorbidities that are weighted differently in the score and it determines the 10 year survival in patients who suffering from multiple comorbidities.
The mortalilty increased with CCI scores: 13.75% (44/320) patients with CCI score of 1-2, 35.93% (115/320) patients with CCI score of 3-4 and 50.31% (161/320) patients with CCI score ≥5.
Among 320 patients 157 has more than (50%) 10 year survival rate and 163 (50%) has less than 10 year survival rate.
When we correlate the outcome (alive or dead) and comorbidities among the total patients it was found to be statistically significant with p<0.05. In the prospective analysis there is no significant difference between the outcome and comorbidities (p>0.05) while in the retrospective analysis there is significant difference (p<0.05).
Table 5. Effect of comorbidities on outcome Prospective Vs Retrospective
|
Study Design |
Cci-Status (Comorbidities) |
Total |
||||
|
Mild |
Moderate |
Severe |
||||
|
Prospective |
Outcome |
Dead |
3 |
9 |
24 |
36 |
|
Alive |
10 |
36 |
35 |
81 |
||
|
Total |
13 |
45 |
59 |
117 |
||
|
Retrospective |
Outcome |
Dead |
3 |
13 |
31 |
47 |
|
Alive |
28 |
57 |
71 |
156 |
||
|
Total |
31 |
70 |
102 |
203 |
||
|
Pearson Chi-Square: Prospective -5.531, Retrospective -6.99; df:2; p value: Prospective - 0.063, Retrospective - 0.030 |
||||||
qSOFA includes 1 point for each of 3 criteria: Respiratory rate (RR)≥ 22bpm, altered mental status(GCS)<15, SBP≤100mmHg. A qSOFA score ≥2 is suggestive of sepsis. It is used to predict the in-hospital mortality. Out of 320 patients 128 patients was associated with not high risk status (qSOFA:0-1), and 192 had high risk status (qSOFA:2-3). qSOFA scores 2-3 are associated with a 3-14 fold increase in the in-hospital mortalilty.
Comparing the outcome and qSOFA risk status among the total patients it was found to be statistically significant (p<0.001) and the same was observed prospectively and retrospectively. A high qSOFA score was associated with increased death rate compared with low qSOFA score.
Table 6. Comparison of qSOFA and outcome Prospective Vs Retrospective
|
Study Design |
Qsofa Risk Status |
Total |
|||
|
Not High Risk |
High Risk |
||||
|
Prospective |
Outcome |
Dead |
4 |
32 |
36 |
|
Alive |
39 |
42 |
81 |
||
|
Total |
43 |
74 |
117 |
||
|
Retrospective |
Outcome |
Dead |
1 |
46 |
47 |
|
Alive |
84 |
72 |
156 |
||
|
Total |
85 |
118 |
203 |
||
|
Pearson Chi-Square:Pros-14.708, Retro-36.693; Df:1; P Value: <0.001 |
|||||
Drug related problems
The prevalance and type of drug related problems (DRPs) were studied using the Pharmaceutical Care Network Europe (PCNE) classification system10 and Adverse Drug Reaction (ADR) was assessed by using the Naranjo algorithm.
From the 320 patients analysed 91 (28.43%) patients had drug related problems (DRPs). A total of 104 DRPs were identified. The three leading categories of DRPs found to be untreated indication-29 (31.86%), drug interaction-26 (28.57%) and adverse drug reaction-24 (26.37%).
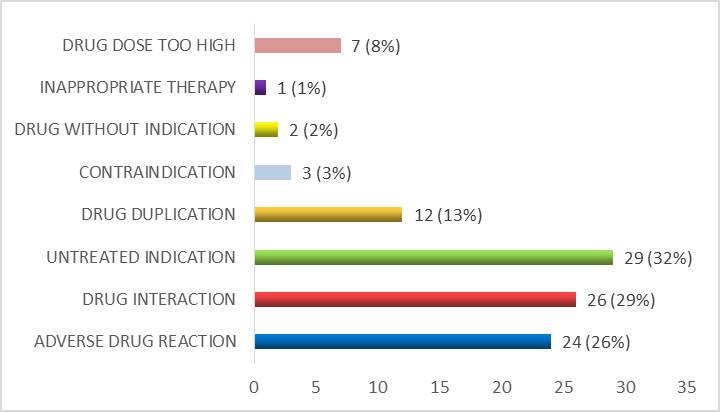
Figure 6. Drug related problems identified in the study population
Among the untreated indications anemia was the leading one, then cefuroxime was found to be more in causing drug interations, adverse drug reactions was most frequently reported with furosemide, drug duplication(13%) mostly with doxofylline, meropenem was associated with drug dose too high(8%) and other DRPs include contraindication(3%), drug without indication(2%), and finally inappropriate therapy (1%).
Based on the causality assessment of ADRs using Naranjo’s Causality Assessment Scale, out of 24 ADRs identified in the study population (8 prospectively and 16 retrospectively), 17 ADRs were found to be probable (5 prospectively and 12 retrospectively), 7 ADRs were possible (3 prospectively and 4 retrospectively). No ADRs were classified as definite or doubtful in the study population.
In the prospective analysis out of 117 patients 34 (29.05%) patients were identified with DRPs among which drug interaction -11 (32.35%) was the most commonly identified drug related problem followed by untreated indication-8 (23.53%) and adverse drug reaction-8 (23.53%).
In the retrospective analysis out of 203 patients 57 (28.07%) patients were identified with DRPs, among which untreated indication-21(36.84%) was the most frequently identified drug related problem followed by adverse drug reaction-16 (28.07%) and drug interaction-15 (26.3%).
Table 7. Recognized problems based on PCNE DRP classification tool V9.1
|
Primary Domain |
Code V9.1 |
Problem |
Prospective |
Retrospective |
|
Treatment effectiveness |
P1.1
P1.2
P1.3 |
No effect of drug treatment despite correct use Effect of drug treatment not optimal Untreated symptoms or indication |
0
0
8
8
0
0 |
0
0
21
16
0
0 |
|
Treatment safety |
P2.1 |
Adverse drug event (possibly) occurring |
||
|
Other |
P3.1
P3.2 |
Unnecessary drug-treatment Unclear problem/complaint. |
Table 8. Recognized causes based on PCNE DRP classification tool V9
|
Primary Domain |
Code V9.1 |
Prospective |
Retrospective |
|
Drug Selection |
C1 |
5 |
13 |
|
Drug Form |
C2 |
0 |
0 |
|
Dose Selection |
C3 |
3 |
4 |
|
Treatment duration |
C4 |
0 |
0 |
|
Dispensing |
C5 |
0 |
0 |
|
Drug use process |
C6 |
0 |
0 |
|
Patient related |
C7 |
0 |
0 |
|
Patient transfer related |
C8 |
0 |
0 |
|
Others(Drug Interations) |
C9 |
11 |
15 |
Discussion
We included a total of 320 patients, among which 117 was analysed prospectively and 203 retrospectively. While considering the overall population elderly patients was more likely to have sepsis compared with middle aged and younger adults. Similarly the study conducted by Martin et.al concluded that the incidence of sepsis is higher in elderly when compared with younger sepsis patients (Martin et al., 2006) and the incidence of sepsis is more common in male sex which correlates with the study done by Yasser Sakr et.al (2013).
In this study the management of sepsis was evaluated by considering the Fluid therapy, Antimicrobial therapy (Antibiotics & Antifungals), Vasopressor therapy and Blood component therapy. In general normal Saline was the most commonly administered fluid (90.13%), prospectively (91.96%) as well as retrospectively (89.11%). From a study conducted by Chien-Hua Tseng et al, it was found that normal saline was the mostly administered IV fluid (Tseng et al., 2021). Then considering the antibiotic therapy cefoperazone-sulbactum (50.63%) was the most commonly prescribed one, same was observed prospectively (75%) and retrospectively (80%). A study was conducted by Harlan Stone et al, showed that third generation cephalosporins were associated with more cure rate compared with other class of antibiotics (Stone et al., 1983). Fluconazole was the most frequently administered antifungal in general (64%), prospectively (55%) and retrospectively (68%). A study conducted in 2014 by Winnie Lee et al, out of 233 patients screened two-third of the patients were given fluconazole (66.67%) (Lee et al., 2014). On evaluating vasopressor therapy noradrenaline (67.12%) was the predominent one generally, in prospective (75.86%) and retrospective (61.36%) analysis. In a study conducted by Martin et al, with 97 adult patients with septic shock, noradrenaline was the most predominently used vasopressor agent and significantly lower the mortalilty rate compared with other agents (Martin et al., 2000). Finally Packed Red Blood Cells (PRBC) was the most commonly administered blood component therapy (83.99%), prospectively (75.51%) and retrospectively (88%). Adherence to the SSC international guidelines-2016 was assessed through 3-Hour and 6-Hour bundles. On analyzing the 3-Hour compliance 64.1% and 60.6% adherence to the guideline was found out in the prospective and retrospective analysis respectively. Out of 320 patients 61.9% compliance was obtained. On evaluating the 6-Hour compliance 87.2% and 84.2% adherence to the guideline was identified in the prospective and retrospective analysis and among total patients it was obtained as 85.3%. Subjective to our analysis out of 320 patients 184 (57.5%) were explored with both 3-Hour and 6-Hour compliance. From a study conducted by Andrew Rhodes et al (2015), showed that adherence to the 6 hour bundle is more when compared with 3 hour bundle. A similar result was observed in our study also.
While categorizing the “stages of sepsis” as sepsis, severe sepsis and septic shock, the incidence of “sepsis” was found to be higher. Among the total study population it was 43% and in prospective analysis (47%), but in retrospective analysis severe sepsis (41.4%) was prominent. From a study conducted by Salvo et al, revealed that incidence of sepsis was greater when compared with other two categories (Salvo et al., 1995).
Then analysing the causative organisms bacteria (52%) was the mostly isolated pathogen in the study population and also prospectively and retrospectively. Urinary Tract Infection-141 (44.06%) was the most predominent focus of infection in which E. Coli-71(22.18%) was the frequently isolated pathogen.
When correlating the CCI Score status (comorbidities) and outcome (alive or dead) significant association was observed on an average (p value: 0.003) as well as retrospectively (p value: 0.030), but not in prospective (p value: 0.063) analysis. A study conducted by Yong Yang et al, demonstrated that effect of comorbidities and in-hospital mortalilty was significant (Yang et al., 2010). Then comparing the Quick Sequential Organ Failure Assessment (qSOFA) risk status (mortality) and outcome among the total patients it was found to be statistically significant and the same was observed prospectively and retrospectively (p value : 0.000). From a study conducted by Kristina E. Rudd et al, shown that high qSOFA score was associated with increased death rate compared with low qSOFA score. A similar result was observed in our study also (Rudd et al., 2018).
Out of 320 patients a total of 104 drug related problems(DRPs) were identified in 91(28.43%) patients, among which the three leading categories of DRPs found to be untreated indications-29 (31.86%), drug interactions-26 (28.57%) and adverse drug reactions(ADRs)-24 (26.37%). Drug interactions-11(32.35%) and untreated indications-21(36.84%) were the mostly occured DRPs in prospective and retrospective analysis respectively. A study conducted by Firomsa Bekele et al, showed that untreated indication was the widely occured drug related problem. A similar result was observed in our study also (Bekele et al., 2021).
Limitation of the study
Some of the limitations of ours study must be acknowledged. First, the study was limited to only bacterial and fungal sepsis so could not assess the viral sepsis and its management. Second, Azoles were the only class of antifungals obtained in our study therefore other class could not be studied. Third, the study was single centered which deprive the generalizability of the study to different populations and centers. Fourth due to the pandemic situation, drug related problems are only identified and categorised, could not make any interventions.
Conclusions
In our study the management of sepsis is done thoroughly with timely fluid therapy, antimicrobial therapy, blood component and vasopressor therapy. Overall analysis indicates that; in the fluid therapy - normal saline, antibiotic therapy - cephalosporins (cefoperazone-sulbactum), antifungal therapy - azoles (fluconazole), blood component therapy - PRBC, and vasopressor therapy - noradrenaline were mostly observed. Adherence to SSC Guidelines-2016 ( both 3-Hour and 6-Hour bundles) was found to be 57.5%. Incidence of “Sepsis" was the highest during the categorization of the stages of sepsis. UTI was the predominent focus of infection in which E. Coli was the frequently isolated pathogen. Statistically significant association was observed between comorbidities and outcome as well as mortality rate and outcome. Untreated indication was the frequently identified DRPs in which anemia was more often.
Acknowledgement
The authors are thankful to the Department of Pharmacy Practice, St. Joseph’s College of Pharmacy- Alappuzha and Lourdes Hospital- Ernakulam, Kerala, India
Conflicts of interest: Nil
References
Bekele F, Fekadu G, Bekele K, Dugassa D, Sori J. 2021. Drug-related problems among patients with infectious disease admitted to medical wards of Wollega University Referral Hospital: prospective observational study. SAGE open medicine, 9, 2050312121989625.
CDC. 2022. What is sepsis? Centers for Disease Control and Prevention: https://www.cdc.gov/sepsis/what-is-sepsis.html
Gyawali B, Ramakrishna K, Dhamoon AS. 2019. Sepsis: The evolution in definition, pathophysiology, and management. SAGE Open Medicine, 7: 2050312119835043.
Husabø G, Nilsen R M, Flaatten H, Solligård E, Frich JC, Bondevik GT, Hovlid E. 2020. Early diagnosis of sepsis in emergency departments, time to treatment, and association with mortality: an observational study. PLoS One, 15(1):e0227652.
Lee W, LiewY, Chlebicki MP, Ong S, Lee P, Kwa A. 2014. An observational study on early empiric versus culture-directed antifungal therapy in critically ill with intra-abdominal sepsis. Critical Care Research and Practice, 2014:479413.
Martin C, Viviand X, Leone M, Thirion X. 2000. Effect of norepinephrine on the outcome of septic shock. Critical Care Medicine, 28(8):2758-2765.
Martin GS, Mannino DM, Moss M. 2006. The effect of age on the development and outcome of adult sepsis. Critical Care Medicine, 34(1):15-21.
Milano PK, Desai SA, Eiting EA, Hofmann EF, Lam CN, Menchine M. 2018. Sepsis bundle adherence is associated with improved survival in severe sepsis or septic shock. Western Journal of Emergency Medicine, 19(5):774.
Negret-Delgado MDP, Puentes-Corredor S, Oliveros H, Poveda-Henao CM, Pareja-Navarro PA, Boada-Becerra NA. 2016. Adherence to the guidelines for the management of severe sepsis and septic shock in patients over 65 years of age admitted to the ICU. Colombian Journal of Anestesiology, 44(4): 299-304.
O’Connell K, Vandergriendt C. 2021. Sepsis: Symptoms, causes, treatment, risks, and more. Healthline. https://www.healthline.com/health/sepsis
PCNE Classification for Drug-Related Problems V9.1 -Page 1 Classification for Drug related problems. Pcne.org. [cited 2022 Jun 15]. Available from: https://www.pcne.org/upload/files/417_PCNE_classification_V9-1_final.pdf
Rhodes A, Phillips G, Beale R, Cecconi M, Chiche JD, De Backer D, Levy M. 2015. The surviving sepsis campaign bundles and outcome: results from the international multicentre prevalence study on sepsis (the IMPreSS study). Intensive Care Medicine, 41:1620-1628.
Rudd K E, Seymour CW, Aluisio A R, Augustin ME, Bagenda DS, Beane A, Angus, D C. 2018. Association of the quick sequential (sepsis-related) organ failure assessment (qSOFA) score with excess hospital mortality in adults with suspected infection in low-and middle-income countries. JAMA, 319(21):2202-2211.
Ryding S, Lois Zoppi BA. 2018. The stages of sepsis. News-Medical.net. Available from: https://www.news-medical.net/health/The-Stages-of-Sepsis.aspx
Sakr Y, Elia C, Mascia L, Barberis B, Cardellino S, Livigni S, Fiore G, Filippini C, Ranieri VM. 2013. The influence of gender on the epidemiology of and outcome from severe sepsis. Critical Care, 17(2):1-9.
Salvo I, De Cian W, Musicco M, Langer M, Piadena R, Wolfler A, Sepsis Study Group. 1995. The Italian SEPSIS study: preliminary results on the incidence and evolution of SIRS, sepsis, severe sepsis and septic shock. Intensive care medicine, 21, S244-S249.
Stone HH, Strom PR, Fabian TC, Dunlop WE. 1983. Third-generation cephalosporins for polymicrobial surgical sepsis. Archives of Surgery, 118(2):193-200.
Surviving Sepsis Guidelines' Criteria for Sepsis Diagnosis (https://pulmccm.org/review-articles/surviving-sepsis-guidelines-criteria-diagnosis-sepsis/)
Tseng CH, Chen TT, Chan MC, Chen KY, Wu SM, Shih MC, Tu YK. 2021. Impact of Comorbidities on Beneficial Effect of Lactated Ringers vs. Saline in Sepsis Patients. Frontiers in Medicine, 8: 758902.
Yang Y, Yang KS, Hsann YM, LimV, Ong BC. 2010. The effect of comorbidity and age on hospital mortality and length of stay in patients with sepsis. Journal of critical care, 25(3), 398-405.







