Hemalatha B.1 , Jeevika V. M.1 , Julega K. S.1 , Mohankumar M.2* , Venkateshan N.3
1Doctor of Pharmacy, Arulmigu Kalasalingam College of Pharmacy, Krishnan Koil, Tamil Nadu, India
2Assistant Professor, Department of Pharmacy Practice, Arulmigu Kalasalingam College of Pharmacy, Krishnan Koil, Tamil Nadu, India
3Professor, Department of Pharmaceutical Chemistry , Arulmigu Kalasalingam College of Pharmacy, Krishnan Koil, Tamil Nadu, India
*Address for Corresponding Author
Dr. Mohankumar M.
Assistant professor,
Department of Pharmacy Practice, Arulmigu Kalasalingam College of Pharmacy, Krishnan Koil – 626 126, Tamil Nadu, India
Abstract
Background: Schizophrenia is a chronic heterogeneous syndrome of delusion, Hallucination, disorganized and bizarre thoughts, cognitive deficits and impaired psychosocial functioning Objective: The objective of the study is to evaluate the efficacy among antipsychotic drugs and assess the demographic details, clinical characteristics of schizophrenia. Materials and Methods: A prospective observational study was conducted in a tertiary care hospital, Virudhunagar. Results: A total of 50 patients were enrolled in the study. Out of 50, males were 28 (56%) and females were 22 (44%) Majority of the patients were in the age group of 28-38 years (50%) followed by 18-28 years (50%), 38-48 (6%) and 48-60 years (4%). In this study SES (socio economic scale) was classified according to modified kuppuswamy scale 2019 and the majority of patients were from Upper lower (32%) followed by Upper middle (28%), Lower middle (28%) and lower (12%). Most number of patients were admitted with complaints of both positive (hallucinations and delusions) and negative (flat effect and alogia) (60%) and followed by positive (16%), positive and cognitive (12%), positive, negative and cognitive (12%). Risperidone was most prescribed drug followed by combined drugs of THP and diazepam (66%) Risperidone reduce positive and negative symptoms compared to other Psychotic drugs. Olanzapine reduce the General Psychopathology symptoms compared to other psychotic drugs and shows statistically difference between the baseline and discharge time that was confirmed by using PANSS. Conclusion: Risperidone reduce both positive and negative symptoms compared to other antipsychotics and improves the patient’s quality of life.
Keywords: Schizophrenia, antipsychotic drugs, hallucination, risperidone, kuppuswamy scale
Introduction
Schizophrenia is a persistent, severe mental condition that causes a loss of reality awareness and a variety of symptoms with unclear causes, most of which are characterized by the presence of psychotic symptoms (Insel, 2010). It is a widespread, terrible, and debilitating mental disorder that usually affects adolescents while they are transitioning into adulthood (Andreasen, 1999). There is no one or single etiological factor that causes schizophrenia. A genetically predisposed person experiences the illness when they are exposed to one of the various environmental stressors.Despite the fact that the precise origin of schizophrenia is still unknown, it may be linked to an abnormally high level of dopamine-dependent neuronal activity (Seeman, 1987). There are four primary dopamine pathways in the brain. The mesolimbic pathway, which controls motivation and desire, the mesocortical pathway, which aids in emotion regulation, the nigrostriatal pathway, which contains motor neurons that bypass the medullary pyramids, to control involuntary movements, and the tuberoinfundibular pathway, which releases dopamine to reduce prolactin secretion, are the other pathways that make up this system. Dopamine levels that are abnormal in schizophrenia mostly impact the mesolimbic and mesocortical circuit (Grace, 2016). Clinical observations are used to make a diagnosis based on the kind of symptoms experienced, their length and intensity, and how the patient's life has changed. Schizophrenia is a clinical diagnosis based on the DSM-5 criteria (Diagnostic and statistical manual of mental disorder ). Disorganised, paranoid, catatonic, undifferentiated, and residual schizophrenia categories, which were formerly listed in the DSM-IV, are no longer considered to accurately represent the heterogeneity of schizophrenia (McCutcheon et al., 2020). Positive symptoms such as hallucinations, delusions, disorganised speech, and disorganised behaviour and negative symptoms of schizophrenia e.g. flat affect, avolition, anhedonia, poor attention, and alogia are observed (Miller et al., 1999). The PANSS (Positive and Negative Syndrome Scale) was used to evaluate people who had been diagnosed with schizophrenia (Kay et al., 1987). Relapse prevention, acute exacerbations, and first episode psychosis are all treated with a multimodal therapy strategy that includes both pharmacological and psychosocial therapies (Maroney, 2020). Educational, psychological, social, and physical treatments are all part of non-pharmacological therapy for schizophrenia (Stevovic et al., 2022).
Materials and methods
Study Design
The study was carried out in Psychiatric Department of Government Medical College Hospital, Virudhunagar. This prospective Observational study was conducted over a period of 6 months. The aim of the study is to evaluate the efficacy among antipsychotic drugs and demographics details, clinical characteristics of schizophrenia.
Study Population
A prospective observational study is conducted with 50 psychiatric patients in both outpatient and inpatient at psychiatric department.
Study Criteria
Inclusion criteria
Exclusion criteria
Statistical Outcome
Data were collected and analysed using Microsoft Excel and Means are compared and Analysed by using Paired t -Test in SPSS program.
Results and discussion
A total of 50 patients were enrolled in the study. Out of 50, males were 28 (56%) and females were 22 (44%) shown in Figure 1 which was similar to the findings of (DeLisi, 1992). Majority of the patients were in the age group of 28-38 years (50%) followed by 18-28 years (50%) , 38-48 (6%) and 48-60 years (4%) shown in figure 2 which correlates with (Hafner et al., 1993). In this study Socio economic status was classified according to modified kuppuswamy scale 2019 and figure 3 shows the majority of patients were from Upper lower (32%) followed by Upper middle (28%), Lower middle (28%) and lower (12%). Majority of the patients were from Rural areas (64%) followed by Semi Urban areas (36%) shown in Figure 4. Idiopathic (36%) is the primary cause followed by family history (22%), alcohol (20%), cannabis use (14%) and child abuse (8%) depicted in figure 5 and which resembles the findings in (John H. Gilmore, 2010). Majority of the patient had duration of 9 days (16%) followed by 5 days and 10 days(14%),7 days (12%),8 days and 6 days (8%) 13 and 15 days (6%)11,12 and 14 days (4%) and 16 and 18 days (2%) shown in Table 1 and Figure 6. Most number of patients were admitted with complaints of both positive (hallucinations and delusions) and negative (flat effect and alogia) (60%) and followed by positive (16%), positive and cognitive (12%), positive, negative and cognitive (12%) are shown in Table 2 and Figure 7. Table 3 and Figure 8 shows the categories of drugs prescribed in higher numbers are Risperidone (52%), followed by haloperidol (24%), olanzapine (12%) and chlorpromazine (10%). Supportive therapy prescribed as combined drugs are THP and diazepam (66%), THP and clonazepam (8%) and monotherapy are THP (20%) followed by diazepam (6%) are shown in Table 4 and Figure 9. Table 5 listed the efficacy of prescribed drugs were assessed by using Positive and negative syndrome scale at baseline and discharge time and it revealed that there is statistically significance difference between symptoms of patients on baseline and discharge time. Risperidone reduce positive and negative symptoms compared to other antipsychotic drugs which was similar to the findings of (Saeed shoji shafti, 2014) .Olanzapine reduce the General Psychopatholgy symptoms compared to other psychotic drugs and the result is significant at p<0.05.
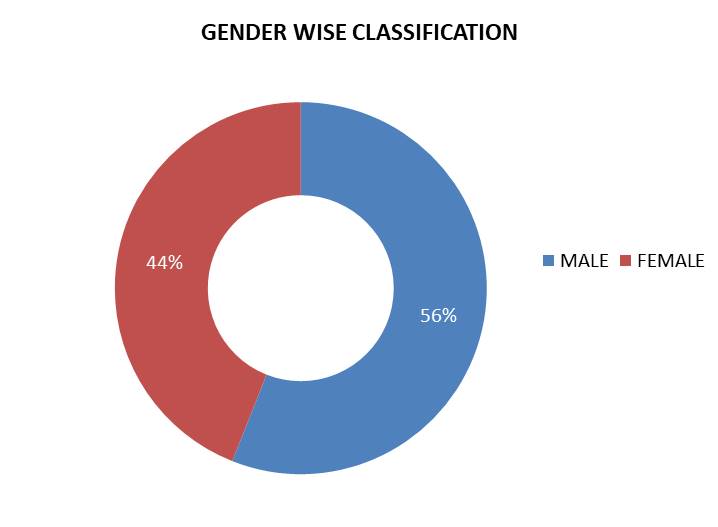
Figure 1. Gender wise classification
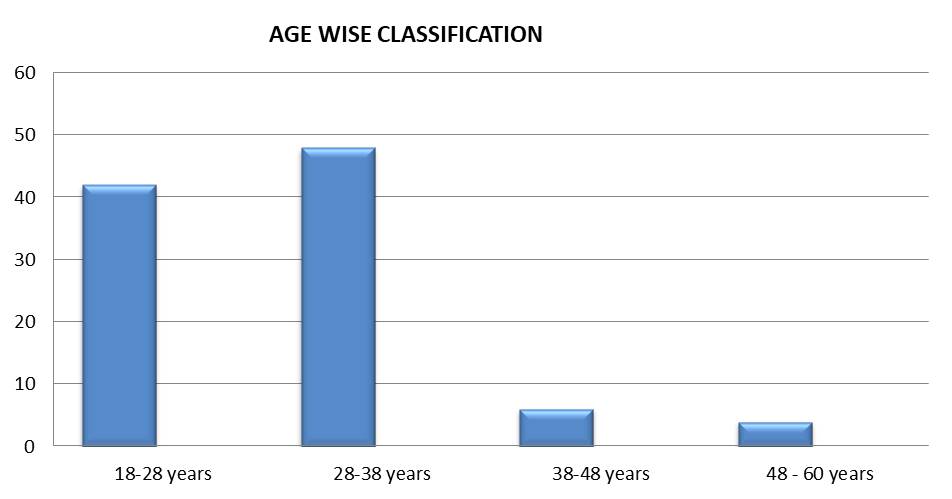
Figure 2. Age wise classification
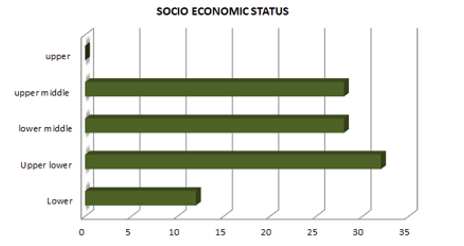
Figure 3: Socio economic status
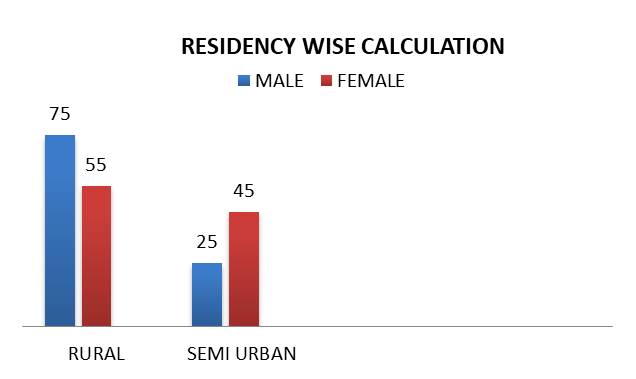
Figure 4: Residency wise calculation

Figure 5: Duration of stay
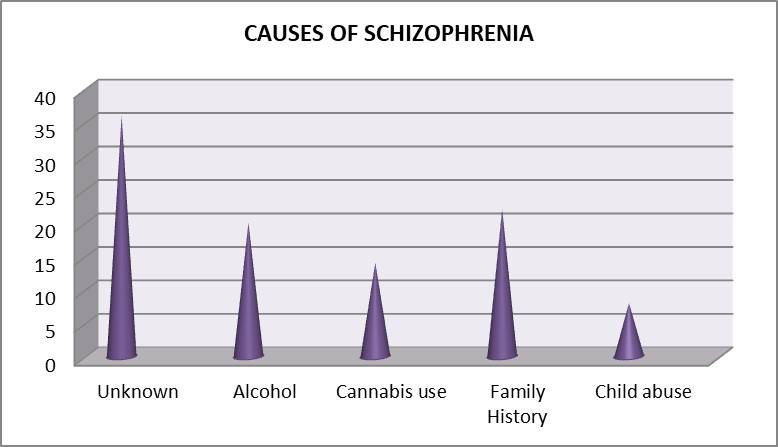
Figure 6: Causes of schizophrenia
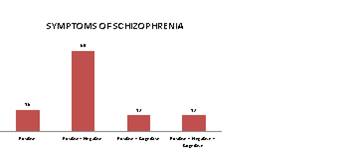
Figure 7: Symptoms of schizophrenia
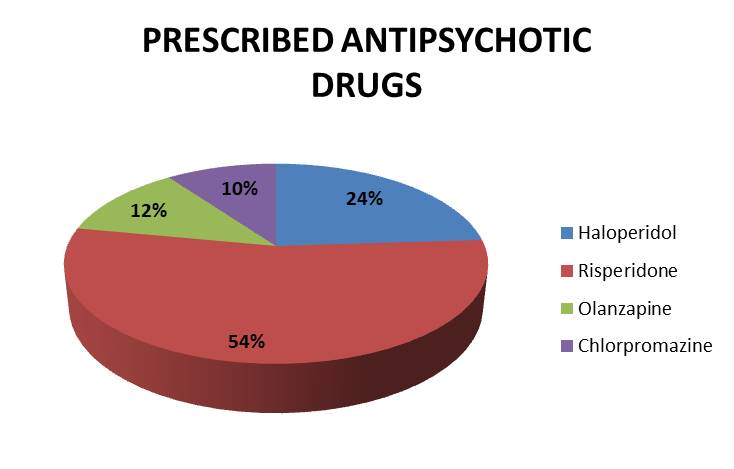
Figure 8: Prescribed antipsychotic drugs
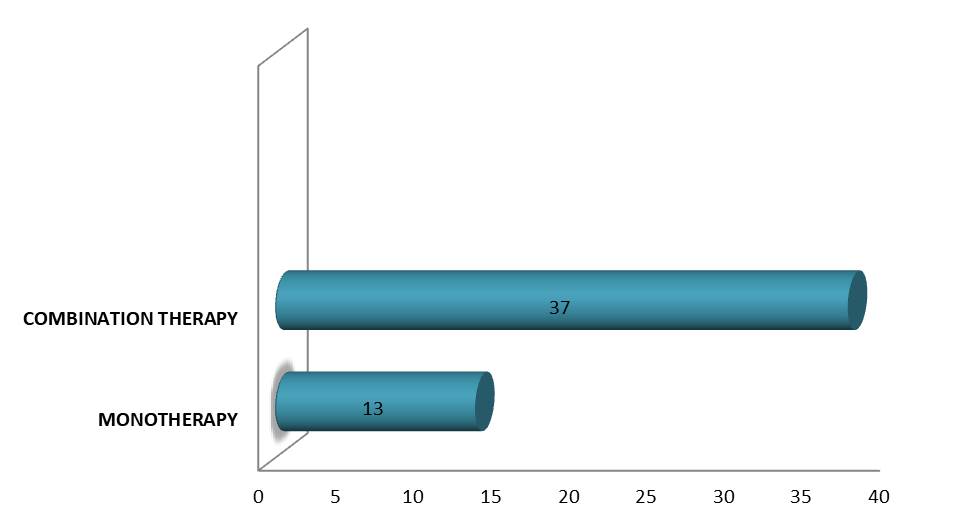
Figure 9. Supportive therapy
Table 1. Duration of stay
|
No of days |
No of patients (N =50) |
Percentage % |
|
5 Days |
7 |
14 |
|
6 Days |
4 |
8 |
|
7 Days |
6 |
12 |
|
8 Days |
4 |
8 |
|
9 Days |
8 |
16 |
|
10 Days |
7 |
14 |
|
11 Days |
2 |
4 |
|
12 Days |
2 |
4 |
|
13 Days |
3 |
6 |
|
14 Days |
2 |
4 |
|
15 Days |
3 |
6 |
|
16 Days |
1 |
2 |
|
18 Days |
1 |
2 |
Table 2. Symptoms of schizophrenia
|
Symptoms |
No of patients (N = 50) |
Percentage (%) |
|
Positive |
8 |
16 |
|
Positive+ Negative |
30 |
60 |
|
Positive + Cognitive |
6 |
12 |
|
Positive + Negative + Cognitive |
6 |
12 |
Table 3. Prescribed antipsychotic drugs
|
Name of drugs |
No of patients (N = 50) |
Percentage % |
|
Haloperidol |
12 |
24 |
|
Risperidone |
27 |
54 |
|
Olanzapine |
6 |
12 |
|
Chlorpromazine |
5 |
10 |
Table 4. Supportive therapy
|
Therapy |
Drugs |
No of patients (N =50) |
Percentage % |
Total N = 50 |
|
Monotherapy |
Trihexyphenidyl |
10 |
20 |
13 patients |
|
Diazepam |
3 |
6 |
||
|
Combination therapy |
Trihexyphenidyl + Diazepam |
33 |
66 |
37 Patients |
|
Trihexyphenidyl +Clonazepam |
4 |
8 |
Table 5. Efficacy of antipsychotic drugs assessed by PANSS
|
Antipsychotic drug |
Baseline |
Discharge |
t Value |
Difference ( P Value ) |
|
Risperidone ( n=27) |
|
|
|
|
|
Positive |
13.7±2.17 |
10.07±1.49 |
13.929 |
<0.000 |
|
Negative |
13.07±2.43 |
9.40±1.30 |
10.02 |
<0.000 |
|
General Psychopathology |
24.25±2.68 |
19.62±1.69 |
15.065 |
<0.000 |
|
Haloperidol (n=12) |
|
|
|
|
|
Positive |
10.91±1.88 |
8.50±1.31 |
6.751 |
<0.000 |
|
Negative |
10.0±2.95 |
8.58±1.78 |
3.742 |
<0.003 |
|
General Psychopathology |
23.08±2.27 |
20.0±2.21 |
15.976 |
<0.000 |
|
Olanzapine (n=6) |
|
|
|
|
|
Positive |
10.05± 1.04 |
8.33±1.21 |
13.00 |
<0.000 |
|
Negative |
9.0±1.41 |
7.83± 0.75 |
3.796 |
<0.013 |
|
General Psychopathology |
21.33±1.211 |
19.5±1.04 |
3.841 |
<0.012 |
|
Chlorpromazine (n=5) |
|
|
|
|
|
Positive |
10.8±1.92 |
8.80±2.16 |
16.05 |
<0.003 |
|
Negative |
13.0±1.58 |
11.6±2.07 |
7.89 |
<0.025 |
|
General Psychopathology |
22.8±1.92 |
20.0±1.22 |
20.05 |
<0.005 |
*values are mean ±SD n=50
Conclusion
From the study we conclude schizophrenia victimize the male gender high when compared to female gender, but with the slight differences in the age of onset for men early 20s and for female late 20s which was similar to the findings of Patients aged 28-38 are more impact than those of other ages which was similar to the findings of. Patient in Upper lower and rural locality are more affected than those in others. Patient with schizophrenia admitted in hospital in the duration 8-10 days. The most common causes of Schizophrenia are Idiopathic and family history which was similar to the findings of. Patient with schizophrenia mostly get affected by both positive and Negative symptoms than others symptoms. Hallucination and Delusion are more common among other symptoms. First generation antipsychotics (Haloperidol, Chlorpromazine and second generation antipsychotics (Risperidone, Olanzapine) are commonly prescribed drugs followed by supportive therapy of Anticholinergic (THP) and Benzodiazepines (Diazepam). Risperidone reduce positive and negative symptoms compared to other Psychotic drugs , Olanzapine reduce the General Psychopatholgy symptoms compared to other psychotic drugs and shows statistically difference between the baseline and discharge time that was confirmed by using PANSS. The score of PANSS were high at the time of admission, but they gradually return to low after treatment. Pharmacist play on important role to educate about the illness, medication and lifestyle modification to the patient.
Acknowledgement
We would like to express our thanks and gratitude to the guide Prof. Dr. N.Venkateshan, (M. Pharm., Ph. D.) Dr. M. Mohan Kumar (Pharm D.) for sincere guidance and constant encouragement throughout the course of thesis. Our special thanks to the hospital authorities for providing us to access the patient’s medical records.
Conflict of interest
The authors declare no potential conflict of interest
References
Andreasen NC. 1999. Understanding the causes of schizophrenia. New England Journal of Medicine, 340(8):645-7.
DeLisi LE.1992. The significance of age of onset for schizophrenia. Schizophrenia bulletin, 18(2):209-15.
Gilmore JH. 2010. Understanding what causes schizophrenia: a developmental perspective. American Journal of Psychiatry, 167(1):8-10.
Grace AA. 2016. Dysregulation of the dopamine system in the pathophysiology of schizophrenia and depression. Nature Reviews Neuroscience, 17(8):524-32.
Häfner H, Maurer K, Löffler W, Riecher-Rössler A.1993. The influence of age and sex on the onset and early course of schizophrenia. The British Journal of Psychiatry, 162(1):80-6.
Insel TR. 2010. Rethinking schizophrenia. Nature , 468(7321):187-93.
Kay SR, Fiszbein A, Opler LA. 1987. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin, 13(2):261-76.
Maroney M. 2020. An update on current treatment strategies and emerging agents for the management of schizophrenia. American Journal of Managed Care, 26(3 Suppl):S55-61.
McCutcheon RA, Marques TR, Howes OD.2020. Schizophrenia—an overview. JAMA Psychiatry, 77(2):201-10.
Miller TJ, McGlashan TH, Woods SW, Stein K, Driesen N, Corcoran CM, Hoffman R, Davidson L. 1999. Symptom assessment in schizophrenic prodromal states. Psychiatric Quarterly, 70:273-87.
Seeman P. 1987. Dopamine receptors and the dopamine hypothesis of schizophrenia. Synapse 1(2):133-52.
Shoja Shafti S, Gilanipoor M. 2014. A comparative study between olanzapine and risperidone in the management of schizophrenia. Schizophrenia Research and Treatment, 2014.
Stevović LI, Repišti S, Radojičić T, Sartorius N, Tomori S, Džubur Kulenović A, Popova A, Kuzman MR, Vlachos II, Statovci S, Bandati A. 2022. Non-pharmacological treatments for schizophrenia in Southeast Europe: An expert survey. International Journal of Social Psychiatry, 68(5):1141-50.







