Diksha Aghor*, Sandhya Parameswaran
Saraswathi Vidya Bhavan’s College of Pharmacy, Sankara Nagar, Jagadguru Sankaracharya Marg, Kalyan Shil Road, Dombivli East, Thane, Maharashtra 421204, India
*Address for corresponding author
Diksha Aghor
Saraswathi Vidya Bhavan’s College of Pharmacy, Sankara Nagar, Jagadguru Sankaracharya Marg, Kalyan Shil Road, Dombivli East, Thane, Maharashtra 421204, India
Abstract
Migraine is headache occurring only in one side at a time which is extremely painful and many times associated with nausea and vomiting. Exact cause of migraine is still not known but lot of research is going on to identify mechanism of this disease and various novel drugs, diagnostic tests and drug delivery systems. Drugs from natural origin and its potential effect in treatment of migraine as well as drugs from traditional Indian system of medicines is also becoming new important aspect in treatment of migraine. This review article gives an overview about basic pathophysiology, different types of migraine and their symptoms as well as various antimigraine treatments available so far. Worldwide 15% of total population more has various side effects and not all patients responded to the treatment. Frequency of attacks may increase due to overuse of acute headache medications like NSAIDS it results into conversion of acute migraine into chronic migraine. Hence it was important to discover potential targets and novel approach in treatment of migraine. Commonly affects women 19% than men 11%. Migraine most commonly begins from age 15-24 years of age. By globally burden of disease study it was the third highest prevalent neurological disability. Novel therapies like humanized antibodies, targeted 5-HT1F therapies are some of the recent developments in synthetic drugs. As we know since from thousands of years plants with medicinal properties are important for treatment of various diseases in humans as well as animals. Herbal medicines are now in demand as research is going on. Some of the phytochemicals of some plants are important in treatment of migraine as well as advancement in diagnosis also. We will take review of these potential targets, clinical research, diagnostic tests, phytochemicals, ayurvedic knowledge and novel drug delivery system for conventional drugs.
Keywords: migraine, 5-HT1 receptors, CGRP receptors, phytomedicines, novel administration routes
Introduction
Migraine is “hemicrania” means half of the head. According to world health organization (WHO) globally half to quarters of adult aged 18-65 years current headache disorder. Worldwide 15% of total population more commonly affects women 19% than men 11%. Migraine most commonly begins from 15-24 years of age. By globally burden of disease study it was the third highest prevalent neurological disability. Mechanism of migraine is unknown hence not particular one treatment can treat migraine fully. There is lot of research going on to treat the disease so recent advances in research in migraine has been included in this article. By definition migraine is one sided intense headache along with nausea or vomiting, phonophobia, photophobia and increase in the severity of a pain with head movements. It is a painful neurological condition characterized by severe pain on one or both side of head. It is disabling neurovascular disorder which causes decreased quality of life (Nair, 2018).
Pathophysiology of migraine
Migraine is a disorder of serotonergic system. Over-excitability of certain protein causes inflammation which leads to pain in specific area of brain. Activation and sensitization of trigeminovascular system especially trigeminal nociceptive afferents innervating meninges leads to headache. The frequency of migraine attack may vary from person to person and depends upon threshold of susceptibility. It is important to understand the factors influencing migraine pain which are 1. Threshold of person’s susceptibility to a migraine attack. 2. Mechanism that triggers the attack and the associated symptoms (Haanes and Edvinsson, 2019).
Neuroanatomical structure underlying the migraine
Acute migraine attack occurs in context of individual inherent level of vulnerability; when internal or environmental triggers attack are initiated. The various theories involved in mechanism of migraine (Nair, 2018).
Vascular theory: Thomas Willis in 1930 theory, introduced this theory and is based upon dilation of blood vessels of extra cranial (temporal arteries). These patients were treated with ergotamine which relives the pain and decreases the arterial dilation
Neurogenic theory: This theory focuses on relationship between trigeminal nerves and intracranial vessels. The most recent data shows that a migraine attack most likely originates in the hypothalamus and activates trigeminal nucleus caudalis (TNC). Activation of TNC leads to peripheral release of calcitonin gene related peptides CGRP as most promising target for migraine. There is strong involvement of CGRP in pathophysiology of migraine. Three main steps involved in mechanism of migraine are as follows -
1. Activation of trigeminal vascular system. Optic division of trigeminal nerve stimulates most of the anterior structures which leads to pain in anterior as well as posterior region.
2. Cortical depression –Activation of neurons in trigeminal nucleus caudalis results in inflammatory changes in the sensitive meningeal vascular structures that produces headaches in central as well as peripheral reflex mechanisms.
3. Neuronal Sensitization-Increase in response or sensitivity of neurons towards nociceptive stimulation. Symptoms like throbbing pain which alters the normal pain is due to peripheral and central sensatisation.
The migraine attack is initiated with premonitory symptoms and activation of the hypothalamus. Following hypothalamic activation, the trigeminus nucleus caudalis (TNC) is activated. This leads to activation of the trigeminal ganglion (TG), most likely one-sided, and calcitonin gene-related peptide (CGRP) release. The CGRP release, here exemplified at the middle meningeal artery (MMA), leading to vasodilation. Furthermore, CGRP activates the calcitonin receptor-like receptor/receptor activity-modifying protein (CLR/RAMP1, the CGRP receptor) on the Aδ-fiber. The CGRP receptor activates adenylate cyclase (AC), increasing intracellular cyclic adenosine monophosphate (cAMP). The increase in cAMP leads to a hyper-excitability and a hypothesized activation of hyperpolarization-activated cyclic nucleotide-gated (HCN) channels. cAMP increases the open-probability giving an action potential from the Aδ-fiber, which travels back to the TNC and is further sensed as pain. Sensitization of Aδ-fibers might, in addition, lead to normal stimuli, such as touch, being sensed as pain. When CGRP is released, it is observed that middle meningeal vasodilation of arteries occurs in sensory organs which might lead to sensitization. The increase in CGRP could become most of phonotypical changes observe during migraine attack. There are research shows that c-GMP c-AMP and other neuropeptides such as pituitary adenylate cyclase activating peptide (PACAP) can trigger a migraine attack slightly more than 50% of migraineurs. Most recent data shows that potassium channel opener lecromakalim causes migraine pain in 100 % of patients. Preliminary results reported at the Migraine Trust International Symposium (MTIS) in London in 2018 Clinical Trials. gov identifier NCT03228355 Aδ-fibers are known to be high threshold receptors they are only activated by several mechanical stimulation or extreme heat. However, after being activated by CGRP, the threshold for these responses might be lowered and normal touch or hot/cold stimulation could now be perceived as pain. Preventing sensitizing of Aδ neuronal synapses was recently shown to be a possible mechanism of action of the CGRP antibodies. Preventing sensatisation of Aδ-fibers may be a potential target in treatment c-GMP inhibits breakdown of intracellular c-AMP hence it may be concluded that full pathophysiology of migraine can be explain by c-AMP increases alone. Diagrammatic representation of migraine pathophysiology has shown in figure 1 (Haanes and Edvinsson, 2019).
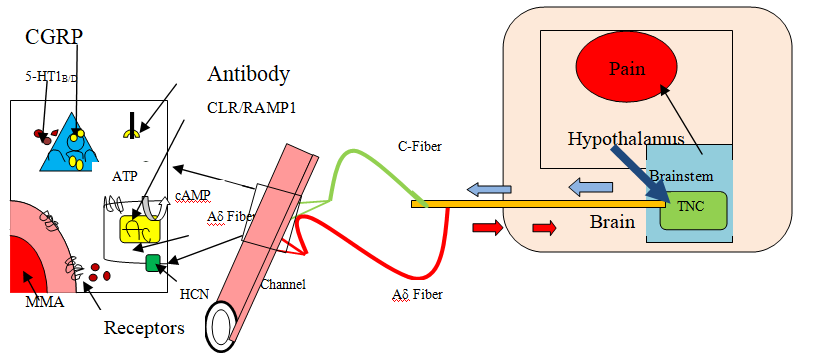
Figure 1. Pathophysiology of migraine
Genetic basis of migraine
It is inherited nature of disorder. Clinical research has shown that with most of patient there is family history of migraine. Transmission of migraine from parents to child is common (Haanes and Edvinsson, 2019).
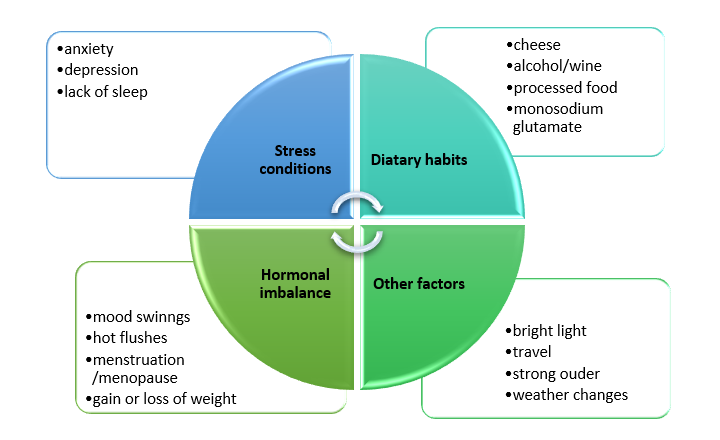
Major trigger facrors
Major trigger factors indicated by (Nair, 2018) are divided into 4 parts and mentioned in figure 2.
Clinical phases with sign and symptoms of migraine
Graphical representation of clinical phases of migraine are as mentioned in figure 3. Migraine pain is many times associated with nausea, vomiting, fever, chills, aching, sweating and sensitivity to light photophobia and sensitivity to sound phonophobia. Clinical phases with sign and symptoms and duration of each phase are mentioned by (blau, 1992) in Table 1.
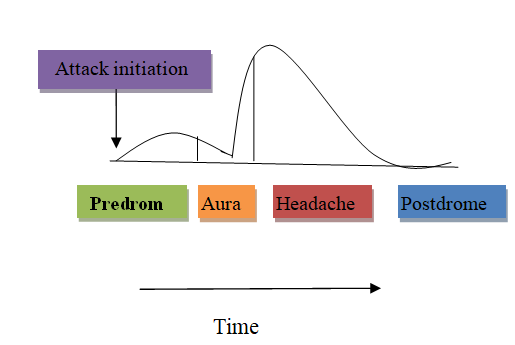
Figure 3. Clinical phases of migraine
Table 1. clinical phases of migraine with duration, sign and symptoms (blau JN, 1992)
|
Sr. No |
Phases |
Duration |
Sign and Symptoms |
|
1 |
Predorme |
Few hours to days before actual pain |
Irritation, depression, excessive sleep, increased urination, muscle stiffness especially neck |
|
2 |
Aura |
5 to 60 minutes |
They are mostly visual, sensory (numbness) or motor in nature and generally lasts than 60 minutes. Visual disturbances are extremely painful with bright flashing lights black spots |
|
3 |
Pain |
4 to 72 hours |
Migraine pain occurs which may be bilateral at onset or gradually start on one side and become generalized usually altering sides from one attack to the next. |
|
4 |
Postdrome |
24 to 48 hours |
Some people feel refreshed or euphoric while others undergo depression or experience tiredness, irritability, mood changes etc. |
Classification of migraine
Different types of migraine their associated symptoms, triggering factors are given as follows in Table 2.
Table 2. Different types of migraine
|
Type of migraine |
Other alternative termed used |
Symptoms, duration and characteristics feature if any |
Associated symptoms |
Triggers |
|
Migraine with aura (Haanes and Edvinsson, 2019) |
- |
Throbbing headache Most prevalent about 70-90% Duration 4-72 hrs |
Nausea, vomiting |
General trigger factors in migraine |
|
Migraine without aura (Haanes and Edvinsson, 2019) |
Classic migraine |
Evolves with sensory isturbances called as aura eg.visual aura |
Blind spots Zigzag lines Numbness weakness in muscles |
Bright light Decrease or ncrease in sleep cycle |
|
Hemiplegic migraine (Haanes and Edvinsson, 2019) |
Variant migraine |
Paralysis on one side of body Familial and poradic are the subtypes Duration -1 hr. to several days |
Speech difficulty Confusion Vision problem |
|
|
Retinal migraine (Nair Sreeja, 2018) |
Ophthalmic or visual migraine |
Very rare 1 in 200 Affects vision of only one eye |
|
Birth control pills Stress, smoking |
|
Chronic migraine (Nair Sreeja, 2018) |
Episodic migraine |
Headache occurs less than 15 times a month |
|
Sleep deprivation Hormonal changes Intake of caffeine |
|
Weekend migraine (Guidotti et al., 2013) |
Let down headache |
It is a headache trigger by change in routine |
Commonly starts at Saturday morning |
Sudden relaxation or reduction in stress level |
Conventional anti migraine drugs.
Ergot alkaloids like ergotamine, dihydroergotamine and methylsageride were used as first generation 5-HT receptors in treatment of migraine. Methylsageride, the first ergot derived prescription drug was used as serotonin 5-HT targeting agent. Lisuride was also used as methylsageride for prophylactic treatment.
5-HT1 receptor and migraine
In 1959, Sicuteri discovered an increase urine excretion of 5-HT1 metabolites during migraine attack, hence 5- Hydroxytriptamine and migraine were linked to each other. Further developments in 5-HT receptor were made in 1990s. (Neeb et al., 2010).
Triptans
Triptans were introduced in 1990s which was major step for migraine therapy. New research focused on formulation of triptans and also its combination with NSAIDS. Triptans are selective 5-HT1B/1D receptor agonists and affinity for 5-HT1F receptors lacks many side effects which are induced due to ergot alkaloids selectively used for migraine. Mechanism of triptans is based on reducing neuroinflammatory release from neurons mainly activation of 5-HT1D and 5-HT1B found within smooth blood vessels. For this reason, triptans is contraindicated in migraine patients with cardiovascular disorders or hypertension. This class is efficient and harmless when given immediately after attack but do not help to reduce other associated symptoms. Conventionally acute attack of migraine attack of migraine is treated with OTC drugs also paracetamol, NSAID’s like aspirin, diclofenac, ibuprofen. Antiemetics are also used like metaclopramide, ondansetron. Currently available triptans are sumatriptan rizatriptan etc. (Neeb et al., 2010) In recent development of non-triptans like Lasmiditan is more selective towards 5-HT1F than 5-HT1B and 5-HT1D receptors (Martha et al., 2013).
Traditional Indian system migraine treatments
Ayurvedic treatment -Ayurveda believes in treating disease in root cause and not just erasing the symptoms some of brief information about some types of therapies used are mentioned in Table 3 (Bisht, 2019).
Table 3. Types of therapies in Ayurveda
|
Shodhana therapy |
Shamana therapy |
Rasa aushadhi |
|
Nasya |
Shirolepa |
Shiravajra rasa |
|
Shiravedha |
Shirobasti |
Ardha nerees rasa |
Need of novel drug therapies in migraine
Even after usefulness of these drugs not all patients responded to triptans adequately. Frequency of attack may increase with overuse of acute headache medication which results into conversion of acute migraine to chronic. 1. As specific acute migraine treatment improved with use of triptans i.e., 5-hydroxytriiptamine (5-HT 1) 2. Many people unaware of migraine headache they tend to take painkillers or NSAIDS which causes conversion of acute migraine to the chronic migraine (Brink et al., 2018).
Different novel drug therapies in treatment of migraine
Development of 5-HT1F Receptor Agonists for Migraine
Ergot and triptans were based on theory of migraine headache which was mainly attributed to abnormal cranial vasodilation. However, some research has revoked this theory and led to conclusion that migraine is neurological disorder and cranial vasodilation may only be a secondary phenomenon due to activation of trigeminal system. Hence need of selective migraine drug or treatment is crucial (Neeb et al., 2010).
Synthetic new drugs in treatment of migraine
Rationale of triptans in migraine is mediated by 5-HT1B/1D receptors and include vasoconstriction of painfully dilated cerebral blood vessels, inhibition of the release of vasoactive neuropeptides by trigeminal nerves, and inhibition of nociceptive neurotransmission. Ditans focus on 5-HT 1F and 5-HT 1D receptor which do not have vasoconstrictive effect out of which 5-HT 1D had been discontinued due to inadequacy. Hence only 5-HT 1F receptors are useful in treatment of migraine with cardiovascular diseases as these receptors do not constricts blood vessels. Preclinical studies have shown that, involvement in modulation of dural neurogenic inflammation and trigeminovascular system establishes potential target for migraine. Hence new class of drugs is characterized as ditans. Three compounds namely, LY 344864, LY334370 and Lasmiditan, but only the last two have been tested in humans. While LY334370 demonstrated a clinical effect in a proof-of-concept study, the development of LY334370 was terminated due to hepatic toxicity in animal models. Lasmiditan, an investigational, oral, first-in-class molecule for the acute treatment of migraine, met its primary endpoint in SPARTAN, a second Phase 3 study. At two hours following the primary dose, a greater percentage of patients treated with Lasmiditan were migraine pain-free as compared to placebo. These results were statistically significant across all three studied doses (50 mg, 100 mg and 200 mg) The approval of REYVOW (Lasmiditan) is critical because it represents the primary new class of acute migraine treatment approved by the FDA in 2019 quite 20 years retrieved by (‘Lilly's REYVOW™ 2019).
Properties of Lasmiditan
Vila-Pueyo, 2018 mentioned the chemical structure of Lasmiditan is different from triptans, thereby is included in a novel drug class defined as ditans. The chemical difference between Lasmiditan and triptans is predicated on the replacement of the indole structure of triptans, which is just like the neurotransmitter 5-HT, by a pyridinoyl-piperidine scaffold.
Although Lasmiditan has more advantages than other synthetic medication, it has some disadvantages, this has been discussed by (Ferrari and Rustichelli, 2021). Advantages like useful in treatment of acute migraine without vasoconstrictive effect but adverse effects like dizziness and parasthesia due to high blood brain barrier penetration are main cause to limitations of Lasmiditan.
A humanized monoclonal anti-CGRP antibodies
CGRP play an important role in migraine pathophysiology. This mechanism has given rise to development of new generation of therapeutics that inhibits interaction of CGRP with its receptors in migraine patients. A new class of such drugs humanized anti CGRP monoclonal antibodies was found effective in reducing frequency of migraine. Fremanezumab (30 mg/kg, IV) clinically, the findings may help to elucidate the therapeutic advantage of CGRP-mAb in reducing headaches of intracranial origin such as migraine with aura and why this therapeutic approach might not be effective for each migraine patient. A CGRP-mAb can prevent the activation and sensitization of high-threshold (central) trigeminovascular neurons by cortical spreading depression, but not their activation from the skin or cornea, suggesting a possible explanation for selectivity to migraine headache, but not other pains, and a predominantly peripheral site of action (Melo et al., 2017).
CGRP receptor antagonist
(Scott, 2020) has given information about Ubrogepant (Ubrelvy™) a novel drug which is a small molecule, highly-selective, calcitonin gene-related peptide (CGRP) antagonist and administered orally. It was developed by Allergan under license to Merck & Co. as an acute treatment for migraine. December 2019, ubrogepant received its first global approval within the USA for the acute treatment of migraine (± aura) in adults. This is the milestone in the development of ubrogepant leading to its first global approval for the acute treatment of migraine (± aura) in adults.
α-6 subunit containing GABAA receptor as novel drug target for inhibition of trigeminal activation
According to (Fan et al., 2018), the α -6 subunit-containing GABAA receptors (α -6GABAARs) are expressed in trigeminal ganglia (TG), the hub of the trigeminal vascular system (TGVS) which is involved in the pathogenesis of migraine. In one of the study researches has been done on α -6 GABAARs. They studied central as well as peripheral TGVS responses induced by capsaicin they got positive results in significantly attenuated the TCC neuronal activation and TG CGRP-ir elevation, and dural CGRP depletion induced by capsaicin. These results suggest that the a6GABAAR in TG is a novel drug target for TGVS activation and that a6GABAAR-selective PAMs have the potential to be developed as a novel pharmacotherapy for migraine.
Phytomedicine involved in migraine treatment
Phytomedicines, or plant-based medicinal formulations, hold great promise in case of the identification of novel therapeutic targets in migraine. Many patients also turn toward herbal and plant-based therapies for the treatment of their migraines as clinical and preclinical evidence of efficacy increases. Patients seek effective and tolerable treatments rather than or additionally to current conventional pharmacological therapies.
phytochemicals in treatment of migraine as mentioned in Table 4.
Table 4. phytochemicals in treatment of migraine.
|
Name of phytomedicine |
Biological source |
Active phytoconstituent in Acting on migraine |
Study design |
Possible Mechanism |
|
Anise oil |
Pimpinella anisum |
Anethole |
Double blind randomised placebo control trials were carried out |
dopamine antagonist could also block the chain of migraine attack cascade ( Mosavat et al., 2019) |
|
combination of Viola odorata, Rosa damascena and Coriandrum sativum |
Iranian traditional medicine |
|
Randomised double blind trial |
effective in improving frequency, duration and severity of migraine attacks (Kamali et al., 2018) |
|
Chamomile oil |
Percian traditional medicine |
Charmazulene Apegenin |
Cross over double-blind trial |
Reduce anxiety associated with headache (Zargaran et al ., 2018) |
|
Rhizome of zingiber |
Zingiber officinalis
|
6 gingerol |
|
Acts as anti-inflammatory (Sharifi-Rad et al., 2017) |
|
Novel Combination of ω-3 fatty acid and nano-curcumin |
|
Curcumin ω-3 fatty acid from food source like fish |
Permuted block randomization |
ω-3 fatty acids block the NFkB signalling pathway, CRP production and proinflammatory cytokine (IL-1β, TNF-α and IL-6) as well as iNOs and COX-2 activity and curcumin has neuroprotective activity combination of these two has shown significant decrease in IL-6 gene expression and CGRP proteins (Abdolahi et al.,2018) |
|
Leaves of abrus Indian liquorice |
Abrus precatorius |
Octadecanoic acid, hexadecanoic acid |
Docking studies were carried out with with CGRP eceptors GCMS and docking analysis |
The comparative analysis of receptor ligand inter-actions showed the potential compounds to target Calcitonin Gene-Related Peptide protein to treat migraine headache (Parthasarathy and Kumar,2019) |
|
Paeonia lactiflora |
Traditional Chinese medicine |
|
intraperitoneal injection (i.p.) of nitroglycerin (NTG, 10 mg/kg) in rats. Pre-treatment with Paeonia lactiflora |
Beneficial for migraine headache treatment. This effect of PL is related to the decrease of c-fos and CGRP in the TNC. (Liao et al.,2019) |
|
Feverfew |
Tanacetum parthenium |
Parthenolide
Chrysanthenyl acetate |
|
Inhibition of platelet aggregation via neutralization of enzyme sulfhydryl Groups Inhibition of prostaglandin synthetase (Rajapakse and Davenport, 2019) |
|
Butterbur
|
Petasites hybridus |
Petasin Isopetasin |
|
Inhibition of leukotriene synthesis in leukocytes Inhibition of voltage-sensitive calcium channels in arterial smooth muscle Cells (Rajapakse and Davenport, 2019) |
|
Cannabis |
Cannabis spp |
Cannabinoids (substituted meroterpenes |
|
Cannabidiol is a lipoxygenase inhibitor that also, like THC, stimulates the release of prostaglandin E2 and inhibits leukotriene B4 synthesis in vitro (Rajapakse and Davenport, 2019) |
|
Saint John’s Wort |
(Hypericum perforatum) |
Hypericin |
|
Counteracts NO donor-induced pain hypersensitivity and meningeal activation by blocking protein kinase C-mediated pathways involving NF-κB, CREB, STAT1 (Rajapakse and Davenport, 2019) |
|
Damask rose
|
(Rosa × damascena) |
Flavonoids Terpenes Myrcene |
|
Analgesic and anti-inflammatory properties, exact mechanism of action Unknown (Rajapakse and Davenport, 2019) |
|
Peppermint |
(Mentha × piperita) |
Methanol |
|
TRPM8 activation with menthol reverses reduced facial pain thresholds induced by meningeal inflammation. (Rajapakse and Davenport, 2019) |
AEA anandamide, CGRP calcitonin gene-related peptide, COX cyclooxygenase, CREB cAMP response element binding protein, NF-κB nuclear factor kappa-light-chain-enhancer of activated B cells, NO nitric oxide, STAT1 single transducer and activator of transcription 1, THC tetrahydrocannabinol, TRPA1 transient receptor potential cation channel subfamily A member 1, TRPM8 transient receptor potential cation channel subfamily M member 8 (Rajapakse and Davenport, 2019).
Emerging role of endocannabinoids in migraine
A new hypothesis on role of cannabinoids in controlling migraine pain which comes under nociceptive migraine pain. Endocannabinoids is comprehensive signalling system present virtually in every cell type and playing critical role in maintaining body homeostasis. Endocannabinoid inhibits neurogenic dural vasodilation mediated by CGRP and NO. Research on (endo) cannabinoids has become relevant once again. Formal approval of a cannabinoid-based drug for other pathologies opens an opportunity for repurposing these agents to treat migraine (Leimuranta, 2018).
Novel diagnostic approaches in detection of migraine
Plasma CGRP as potential biomarkers in diagnosis and therapeutic responses in paediatric migraine
The plasma CGRP level can differentiate migraine from non-migraine headache. It’s going to function as a reference for the therapeutic strategy since it's higher in patients requiring migraine prevention and aware of short-term topiramate treatment. These results are clinically significant, especially for the young children who cannot clearly describe their headache symptoms and should provide new insights into the clinical practice for the diagnosis and treatment of pediatric migraine (Fan et al., 2019).
Identifying menstrual migraine by using statistical method improving a diagnostic criteria
The International Classification of Headache Disorders (ICHD) has diagnostic criteria for menstrual migraine within the appendix. These include the requirement for menstrual attacks to occur within a 5-day window in at least 2/3 menstrual cycles (2/3 –criterion) they employed a simple mathematical model, a Markov chain, to model migraine attacks. A statistical criterion was developed to diagnose menstrual migraine (sMM) and then analyze a knowledge set of migraine diaries using both the 2/3 -criterion and therefore the sMM. At the end of study, they concluded that the ICHD 2/3 -criterion may be a simple screening tool for menstrual migraine, the sMM provides a more specific diagnosis and is able to apply regardless of the number of menstrual cycles recorded. It’s particularly useful for clinical trials of menstrual migraine where an opportunity association between migraine and menstruation must be excluded (Barra et al., 2019).
Animal models used in migraine
Behavioural study of rat model of migraine induced by CGRP.
It is difficult to develop an animal model of migraine that resembles all symptoms of patients. In this study, they established a novel animal model of migraine induced by epidural injection of calcitonin gene-related peptide (CGRP), and examined climbing hutch behavior, facial-grooming behavior, body-grooming behavior, freezing behavior, resting behavior, and ipsilateral hind paw facial grooming behavior of rats following CGRP injection. CGRP significantly reduced climbing hutch behavior, and face-grooming behavior, and increased immobile behavior. They also found that the P15 and P85 percentile range of behavioral data exhibited a high positive rate (83.3%) for establishing the model with less false positive rate. Our results verified that the rat model of migraine induced by CGRP featured many behaviors of migraine patients demonstrated during migraine attacks. These findings suggest that this new model can be a useful tool for understanding the pathophysiology of migraine and studying novel therapeutic strategies for the treatment of migraine. Experimental tools involved in the study of migraine in animals are mentioned in table 5 (Romero-Reyes and Akerman, 2014).
Table 5. Animal experimental tools involved in study of migraine
|
Electrophysiology |
A recording electrode is placed in discrete nuclei in the brain or spinal cord (trigeminocervical complex) and real-time changes in electrical activity (flow of ions) are measured |
|
Intravital video microscopy |
A video microscope is placed over a cranial window to visualize a blood vessel, most commonly the dural middle meningeal artery, and using acquisition hardware and software, changes in the size of the vessel can be determine in response to dural stimulation or chemical mediators |
|
Micro-iontophoresis/ Microinjection |
Used to apply pharmacological agents to discrete areas of the brain. Iontophoresis uses an electric field to charge pharmacological agents in aqueous solution to eject drug and can be combined with a recording electrode to determine the pharmacology of a neuron. |
|
Spontaneous behavioural testing |
Measures spontaneous, non-evoked behaviours that may normally be presented in rodents but may be affected by the study paradigm (noxious stimulation). Comprehends grooming patterns, facial grimace, blinking, exploratory behaviours, rearing, gnawing, freezing, and locomotion |
|
Nitro glycerine induced |
Intravenously or intraperitoneally Mechanical hyperalgesia; thermal and mechanical allodynia; photophobia; meningeal blood flow; reduced locomotor activities; facial expressions of pain |
Scutellaria basicalensis (SB) as an effective traditional Chinese medicine by implication from clinical use and experimental proof using nitroglycerine induced migraine model.
SB is a traditionally used in China for inflammation and as a pain reliever. Recent research is based on effect of SB on migraine. Experimental model using intraperitonial injection of nitroglycerine (NTG) and evaluated using migraine related behavioral test. (Liao et al., 2021) concluded from this study that pretreatment with 1 gm/kg SB relives migraine related behavior in NTG induced migraine model. Hence further clinical studies can be done.
There are various new models and techniques for detection and creation of migraine in animals detail information is given in article ref animal model (Tardiolo, 2019).
Novel drug delivery systems involved in treatment of migraine
Novel intranasal delivery for sumatriptan succinate
Intranasal route is becoming popular choice of drug delivery because prevention from gastrointestinal degradation, first pass metabolism and very good bioavaibility hence Study was done for the preparation and characterization of nasal inserts composing of polyelectrolyte complexes (PECs) based on k-carrageenan (k-CA) and chitosan (CS) to boost therapeutic efficacy of sumatriptan succinate in the treatment of migraine headache. This study illustrates the potential of the lyophilized inserts based on the k-CA/CS PECs, especially k-CA/CS (4:1), for efficient delivery of sumatriptan succinate via the nasal route of administration and suggests a possible therapeutic approach for the termination of migraine attacks (Alavi and Mortazavi, 2018).
Transdermal patches
Rizatriptan is a 2nd generation triptan with lots of benefits over other members of its category. Transdermal patches provide controlled and predetermined. Acceptance and tolerability ratio is high in patients (Ajina et al., 2018).
Chitosan based mucoadhesive polymers
Naturally occurring polymers, particularly of the polysaccharide type, are used pharmaceutically for the delivery of a good sort of therapeutic agents. Chitosan is the second abundant present polysaccharide next to cellulose, which is a biocompatible and biodegradable mucoadhesive polymer that has been extensively utilized in the preparation of micro- and also as nanoparticles. Chitosan micro- or nanoparticles with therapeutic agent-loaded were found to be more stable, permeable, and bioactive. Chitosan based mucoadhesive polymers are used for direct nasal to brain novel drug delivery system. The development of chitosan derivatives has extended these applications due to the enhancement of bioavailability accomplished by an increase in the stability, solubility, mucus adhesiveness, cellular permeability, absorption, biodistribution, and tissue targeting achieved when particulate carriers are based on these derivatives (Ahmed and Aljaeid, 2016).
Receptor activity-modifying proteins (RAMPs)
(RAMPs) interact with G-protein-coupled receptors (GPCRs) to switch their functions, imparting significant implications upon their physiological and therapeutic potentials. Renewing interest in identifying RAMP–GPCR interactions has recently been increased by co evolution studies and orthogonal technological screening platforms. These new studies reveal previously unrecognized RAMP-interacting GPCRs, many of which expand beyond Class B GPCRs. The outcome of these interactions on GPCR function and physiology lays the inspiration for brand fresh molecular therapeutic targets, as evidenced by the recent
success of erenumab (Caron, 2020).
Recent advances in noninvasive neuromodulation using various devices
According to (Angela at el., 2020) Noninvasive neuromodulation is fast growing field which deals with non-pharmacological treatment options for migraine patients. Devices that stimulate peripheral nerves such as vagus nerve, trigeminal sensory nerve, somatic sensory nerve or nerves of brain parenchyma like occipital cortex has been developed for migraine or for prevention of migraine. Currently there are 4 devices which has been approved by US-FDA namely 1. trigeminal nerve stimulator Cefaly 2. Vagus nerve stimulator as GammaCore 3. Transcranial magnetic stimulator is sTMS 4. Nerivio which is a remote electrical neurostimulator. Detail information has given in Table 6.
Table 6. different non-invasive neuromodulation devices.
|
Name of nerve involve in modulation |
Name of device |
US-FDA approval year |
Mode of application |
Mechanism of action |
Safety and efficacy |
|
Trigeminal nerve stimulation |
Cefaly Tech. |
2014 for prevention and 2017 for treatment of migraine |
Electrode applied directly to forehead |
1.modulates trigeminal pathway 2.activates endogenous analgesic pathways through gate control mechanism |
Overall reduction in monthly headache and migraine |
|
Vagus nerve stimulator |
GammaCore |
2017 for acute migraine and 2018 for cluster headache |
Vagus nerve on either side of neck |
It stimulates afferent vagus nerve which interacts with cerebral nuclei in the brain and then undergoes top-down neuromodulation to relieve pain 2.reduces noxious stimuli as well as reduces activity of pronociceptive nuclei |
Clearance by US-FDA for acute migraine but not for prevention Overall safe and well tolerated |
|
sTMS (single pulse transcranial magnetic stimulation) |
sTMS mini |
Only FDA approved device for acute as well as prophylactic treatment |
Rechargeable battery applied to back of the head |
1.stimulates cerebral cortex including currents in cortical neurons and causing neuronal depolarisation 2.may affect neuropeptide release and neuronal plasticity with neuroprotective effect on glial cells Neurotrophic effect on dendritic cells |
No serious adverse reaction found during trials. Safe but not with patients with metal inserted in any operating procedure
|
|
Remote electrical neuromodulation |
Nerivio |
In year 2019 approved for acute migraine |
Applied in upper arm |
1.Induce endogenous analgesia. 2.diffuse noxious inhibitory control |
Early application of device better results within 20 minutes |
Advantages of these devices over internal medication are as follows
1.They are free of side effects.
2.Non-invasive and safe.
Conclusion
This review article has tried to cover every aspect of migraine like its recent research in understanding of pathophysiology, novel drugs including phytomedicines and its potential targets in migraine treatment, recent advancement in diagnostic tests, various techniques and animal model development for experimental based study of migraine therapies. It also includes novel drug delivery systems for better efficiency and tolerability of conventional drugs. This will help for further research in migraine therapies.
References
Abdolahi M, Sarraf P, Javanbakht MH. 2018. A Novel Combination of ω-3 Fatty Acids and Nano-Curcumin Modulates Interleukin-6 Gene Expression and High Sensitivity C-reactive Protein Serum Levels in Patients with Migraine: A Randomized Clinical Trial Study’. CNS Neuronal Disorders Drug Targets, (6):430-438.
Agustin MC, Noseda R, Nir R, Schain A, Stratton J, Strassman A, Burstein R. 2017. Selective Inhibition of Trigeminovascular Neurons by Fremanezumab: A Humanized Monoclonal Anti-CGRP Antibody’. The Journal of Neuroscience, 37(30):7149-7163
Ahmed TA, Aljaeid BM. 2016. ‘Preparation, characterization, and potential application of chitosan, chitosan derivatives, and chitosan metal nanoparticles in pharmaceutical drug delivery’. Drug Design, Development and Therapy, 10:483–507.
Ajina CN, Sandeep DS. 2018. Rizatriptan Transdermal Patches for the Treatment of Migraine. Research Journal of Pharmacy and Technology, 11(3):873.
Alavi S, Mortazavi SA. 2018. Freeze-Dried K-Carrageenan/Chitosan Polyelectrolyte Complex-Based Insert: A Novel Intranasal Delivery System for Sumatriptan Succinate’. Iranian Journal of Pharmaceutical Research, 17(4):1172–1181.
Angela YH, Anna YC, Hsiangkuo Y, Stephen DS. 2019. Peripheral neuromodulation for the treatment of migraine and headache: Recent Advances Bioelectronics in Medicine 2:4, 151-162
Anna F, Cecilia R. 2021. Rational Use of Lasmiditan for Acute Migraine Treatment in Adults: A Narrative Review’, Clinical Therapeutics, 43(4):654–670.
Barra M, Dahl FA, Mac G. 2019. Identifying menstrual migraine-improving the diagnostic criteria using a statistical method. Journal of Headache Pain, 20, 95.
Bisht K. 2019. An ayurvedic approach in the management of migraine: a review study’. Journal of Ayurveda and Integrated Medical Sciences, 4(4):241- 246.
Blau JN. 1992. Migraine: theories of pathogenesis. Lancet; 339(8803):1202-7.
Caron KM. 2020. Dawn of a New RAMPage’. Trends in Pharmacological Sciences, 1692-1709
Chung-CL, Ke-RL, Cheng LL, Jung ML. 2015. The Effectiveness of Scutellaria baicalensis on Migraine: Implications from Clinical Use and Experimental Proof, Evidence-Based Complementary and Alternative Medicine, 1-8.
Fan PC, Kuo PH, Lee MT, Chang SH, Chiou LC. 2019. ‘Plasma Calcitonin Gene-Related Peptide: A Potential Biomarker for Diagnosis and Therapeutic Responses in Pediatric Migraine’. Frontiers in Neurology, 10, 10.
Fan PC, Lai TH, Hor CC. 2018. The α6 subunit-containing GABAA receptor: A novel drug target for inhibition of trigeminal activation’. Neuropharmacology, (140):1-13.
Guidotti M, Barrilà C, Leva S, Piazza D, Claudio, Omboni S. 2013. Symptomatic or prophylactic treatment of weekend migraine: an open-label, nonrandomized, comparison study of Frovatriptan versus naproxen sodium versus no therapy ’Neuropsychiatric Disease and Treatment, (9):81-85.
Haanes KA, Edvinsson L. 2019. Pathophysiological Mechanisms in Migraine and the Identification of New Therapeutic Targets. CNS Drugs (33):525-537.
Jen D. 2019. News release ‘Lilly's REYVOW™ (Lasmiditan), The First and Only Medicine in a New Class of Acute Treatment for Migraine, Receives FDA Approval’, Eli Lilly and Company.
Kamali M, Seifadini R, Kamali H, Mehrabani M, Jahani Y, Tajadini H. 2018. Efficacy of combination of Viola odorata, Rosa damascena and Coriandrum sativum in prevention of migraine attacks: a randomized, double blind, placebo-controlled clinical trial. Electronic Physician, 10(3):6430–6438.
Leimuranta P, Khiroug L, Giniatullin R. 2018. Emerging Role of (Endo)Cannabinoids in Migraine’. Frontiers in Pharmacology. 9, 420.
Liao CC, Li JM, Hsieh CL. 2019. Auricular Electrical Stimulation Alleviates Headache through CGRP/COX-2/TRPV1/TRPA1 Signaling Pathways in a Nitroglycerin-Induced Migraine Rat Model. Evidence-based Complementary and Alternative Medicine.
MaassenVanDenBrink A, Terwindt GM, van den M, AMJM. 2018. Calcitonin gene-related peptide (receptor) antibodies: an exciting avenue for migraine treatment’. Genome Medicine (10):10.
Mosavat SH, Jaberi AR, Sobhani Z, Mosaffa-Jahromi M, Iraji A, Moayedfard. 2019. ‘Efficacy of Anise (Pimpinella anisum L.) oil for migraine headache: A pilot randomized placebo-controlled clinical trial’. Journal of Ethnopharmacology, (236):155-160.
Nair S. 2018. ‘A glance preface and Novel approaches for the efficient treatment of migraine’. International Journal of Research in Pharmaceutical Science, 10(1):282-297.
Neeb L, Meents J, Reuter U. 2010. 5-HT1F receptor agonists: A new treatment option for migraine attacks? Neurotherapeutics, (7):176-182.
Parthasarathy V, Kumar A. 2019. Screening of potential GCMS derived antimigraine compound from the leaves of Abrus precatorius Linn to target “calcitonin gene related peptide” receptor using in silico analysis’ Food Science and Human Wellness, 8:34–39.
Rajapakse T, Davenport WJ. 2019. ‘Phytomedicines in the Treatment of Migraine’. CNS Drugs, 33(5):399-415.
Ramírez Rosas MB, Labruijere S, Villalón CM, Maassen Vandenbrink A. 2013. Activation of 5-hydroxytryptamine1B/1D/1F receptors as a mechanism of action of antimigraine drugs. Expert Opinion on Pharmacotherapy, 14(12):1599–1610.
Romero-RM, Akerman S. 2014. Update on animal models of migraine.’ Current Pain and Headache Reports, 18(11):462.
Scott LJ. 2020. ‘Ubrogepant: First Approval’. Drugs, 80(3):323–328.
Sharifi-RM, Varoni EM, Salehi B. 2017. Plants of the Genus Zingiber as a Source of Bioactive Phytochemicals: From Tradition to Pharmacy, Molecules 22(12):2145.
Tardiolo G, Bramanti P, Mazzon E. 2019. Migraine: Experimental Models and Novel Therapeutic Approaches. International Journal of Molecular Sciences, 20(12):29-32.
Vila-PM. 2018. Targeted 5-HT1F Therapies for Migraine. Neurotherapeutics: the journal of the American Society for Experimental Neurotherapeutics, 15(2):291-303.
Zargaran A, Borhani HA, Salehi-MM. 2018. Evaluation of the effect of topical chamomile (Matricaria chamomilla L.) oleo gel as pain relief in migraine without aura: a randomized, double-blind, placebo-controlled, crossover study’. Neurological Sciences, 39(8):1345-1353.







